
Neurovascular Robotics Heads to the Brain
- Steve Bell

- Dec 1, 2025
- 61 min read
Updated: Apr 22
I know a lot of you reading this will be experts in neurovascular interventions - but I also know for a lot of you this is new. So I want to give a simplified (no one shoot me) backgrounder on what the problem is today that we are trying to fix. I think then the robotic solutions and “Why” will make way way more sense. And I hope we can all agree that this is a massive problem worth solving.

Let me start by saying sorry - as this has become almost a book as I got carried away. But I think it needs explaining in details - read through and then we get to the technology and why it suddenly all makes sense. Stay with it - it’s a meaty read and will have a lot of Typos!
What Is a Stroke?
A stroke is basically a plumbing problem in your brain. Your brain needs a constant supply of blood (that is carrying oxygen and nutrients). If that supply stops, even for a few minutes, brain cells start dying fast. Fast being the important word here.
There are two main types of stroke:
1. Ischaemic Stroke – the blockage (UK Spelling vs Ischemic US)
A blood vessel in the brain gets blocked - usually by a blood clot. Think of it like a pipe with a lump of gunk stuck inside (this is important for later) - it’s like a blocked drain in your home and little to nothing can get past the blockage.The effect: Blood can’t get through and brain tissue downstream starts starving and dying.
This is the most common type of stroke.It’s the one where a mechanical thrombectomy (physically removing the clot) is the lifesaving move.
I want to put this into numbers for you - as you and your family have a high chance of being impacted by a stroke. But let me focus on the more elderly population (where I am rapidly heading to as I age - so all of this is enlightened self interest.)
Let me give you some devastating figures: The annual incidence (new strokes per year) For adults over 60,:
1–2% per year for first-ever ischaemic stroke(That’s 1–2 people out of 100 every year in that age band risk a strike every year.)
But this rises sharply with each decade:m70–79: ~1.5–2% per year80+: ~3–5% per year
By age 60+, roughly 5–10% of the population has already had an ischaemic stroke in their lifetime, depending on: blood pressure, diabetes, obesity, smoking, atrial fibrillation genetics.
By age 80, lifetime prevalence can exceed 15–20%. Yes you read that right!!!!
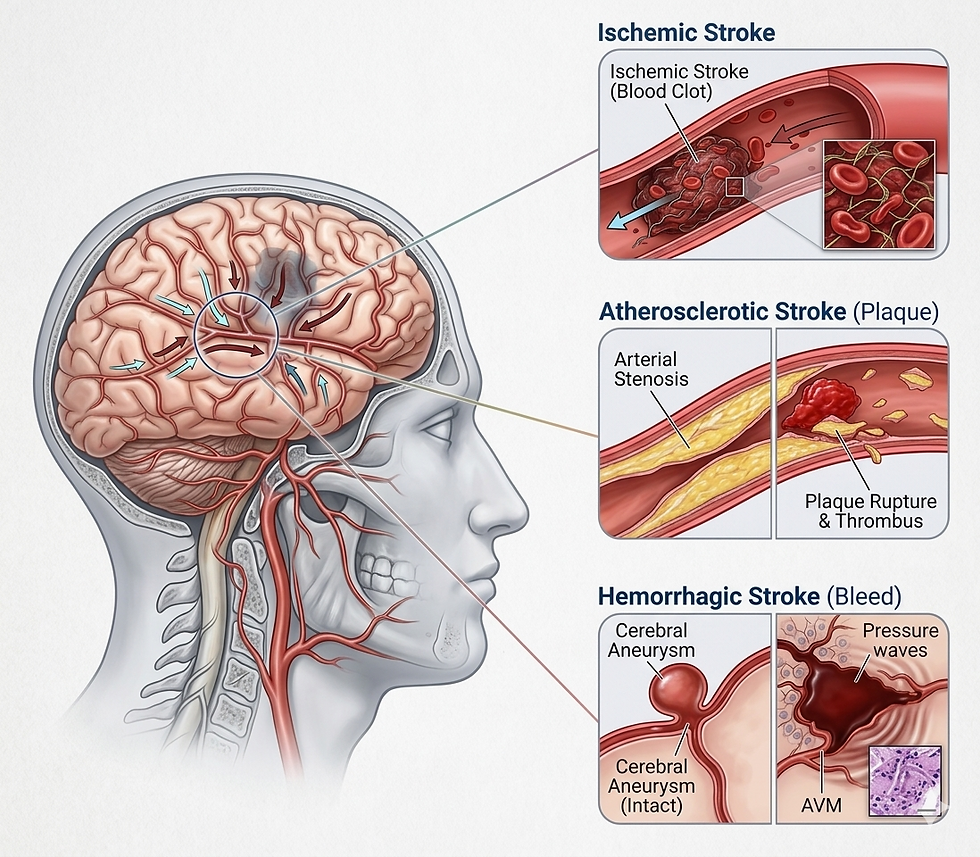
2. Hemorrhagic Stroke – the burst pipe
The second type of stroke is not as common but equally devastating. A blood vessel bursts and blood leaks into the brain. The problem here isn’t lack of blood… it’s blood in the wrong place creating pressure and damage.
This can happen when a vessel wall is weak… which leads us to aneurysms that I’ll cover in a minute.
One important question you need to ask: How Fast Does the Brain Die During a Stroke?
About 1.9 million neurones die every minute. Every F’in minute !!!That’s the number most neurologists use. It’s not poetic exaggeration, it’s modelling based on blood-flow loss during an ischaemic stroke. Let me put that into perspective:
1 minute of delay = a small city’s worth of neurones gone.
10 minutes = almost 20 million neurones.
1 hour = the equivalent of 3.5 years of normal brain ageing.
This is devastating as it hits Cognitive Function
The big problem is that neurones don’t just die randomly - they die in clusters along the affected vessel’s territory. That territory maps to specific abilities, for example:
Speech - Memory - Movement - Vision - Reasoning - and Personality
So the longer the blockage:
the bigger the infarct (the dead tissue),
the more brain networks collapse,
and the greater the permanent disability.
This is why clinicians say: “Time is brain.” It’s not a terrifying slogan - it’s a statistical fact.
It’s really simple…
More minutes = more dead brain = deeper cognitive loss.And once those neurones are gone, the brain cannot regenerate them.
That’s the entire argument for ultra-fast intervention… and why remote and robotic treatment is going to matter so much. Because today, for many people, that ultra fast care is not within reach.
Let me now talk Aneurysm?
An aneurysm is a bulge or balloon in a blood vessel wall. Imagine a weak patch on a bike tyre that slowly balloons out.
Most aneurysms sit there quietly doing nothing and most people are totally unaware they have one. The danger comes if the bulge ruptures.
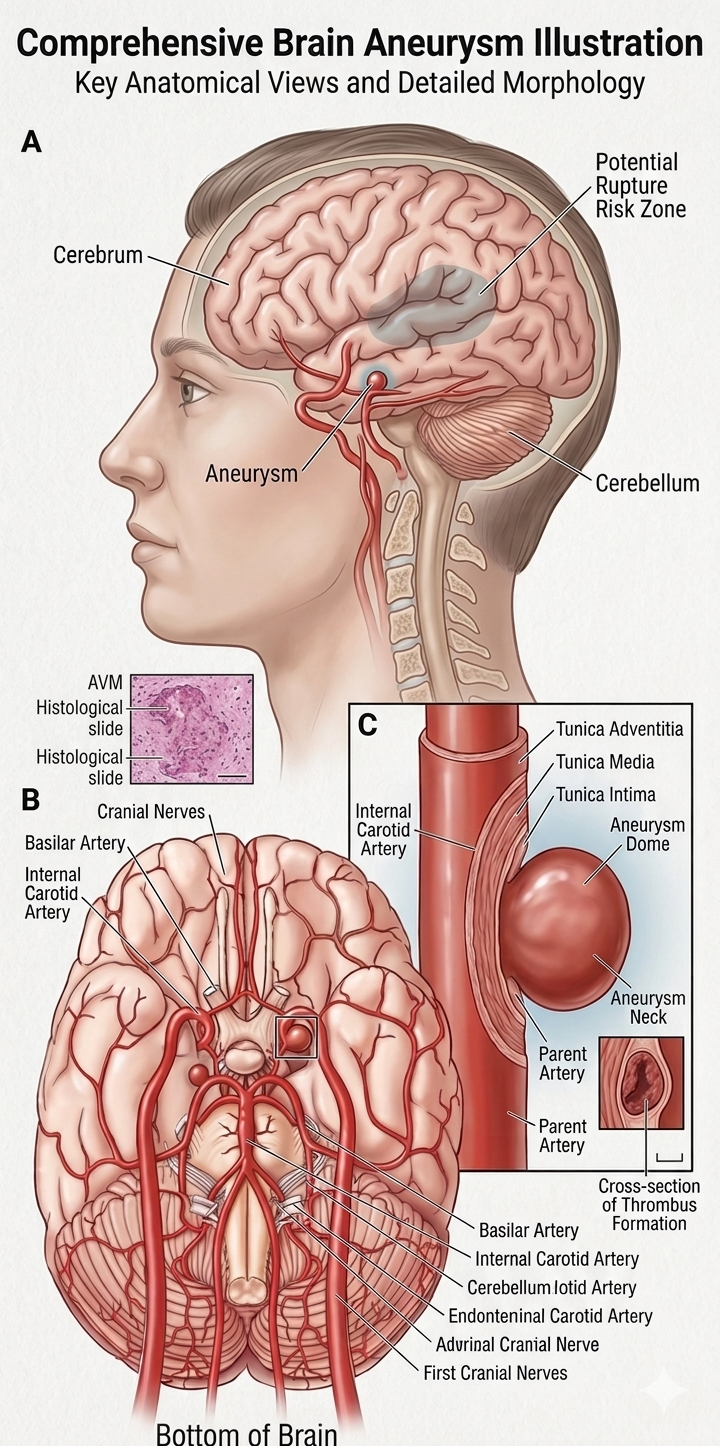
When it bursts, blood pours into the brain - that’s called a subarachnoid haemorrhage - and make no mistake this “brain bleed” is a medical emergency with very high risk.
Treatment usually means:
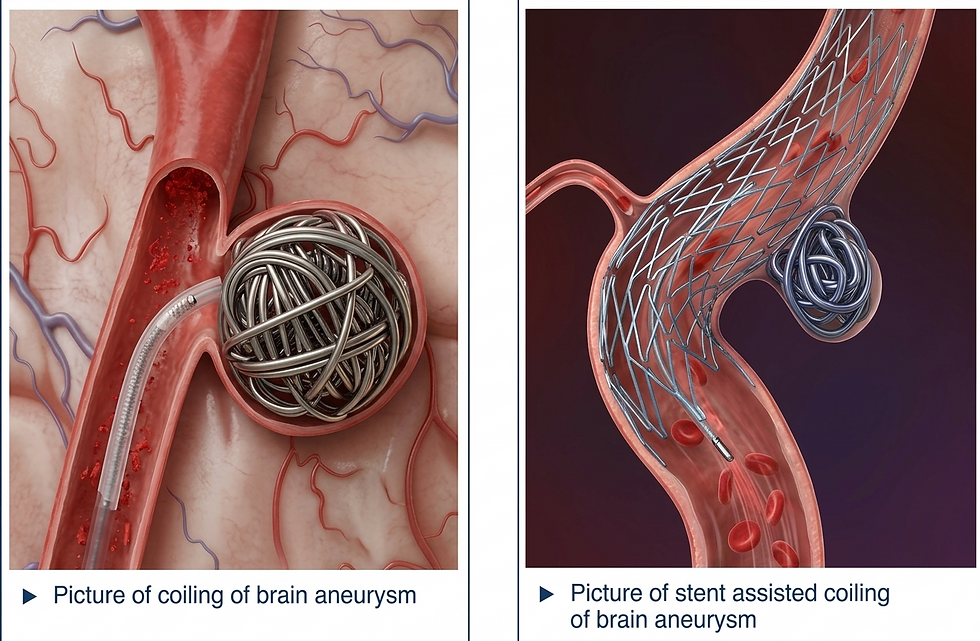
sealing it from the inside with coils (small coiled up metal loops)
or putting a stent or flow diverter across it to stop blood going to the hole
or, in some cases, surgical clipping.
In simple terms:
Stroke (ischaemic): a blocked blood vessel.
Stroke (hemorrhagic): a burst blood vessel.
Aneurysm: a bulging vessel that might burst.
One blocks, one bursts, one threatens to burst.
How are they treated today
Firstly - for those that are surgical operating room centric - let’s talk about site of care - as that is really important later.
Stroke and aneurysm procedures aren’t done “just anywhere.” They require: specialised imaging, highly trained neurointerventionalists, and a controlled catheter-based environment.
So treatments happen in:
Neuro-Interventional Labs (primary)
Biplane IR (Interventional Radiology) Labs (secondary) - biplane meaning two x-ray machines at different angles to get different anatomical views.
Hybrid ORs (special cases) which are like operating rooms with imaging equipment.
Bottom line - you need specialist set ups, equipment and capable staff. And not every small hospital has all of this.
Let me discuss here a little bit generally on how strokes and aneurysms are treated today in an IR Lab as an Interventional Radiology (IR) labs is where the real action happens. Everything before this moment is assessment. This is where the fixing happens.
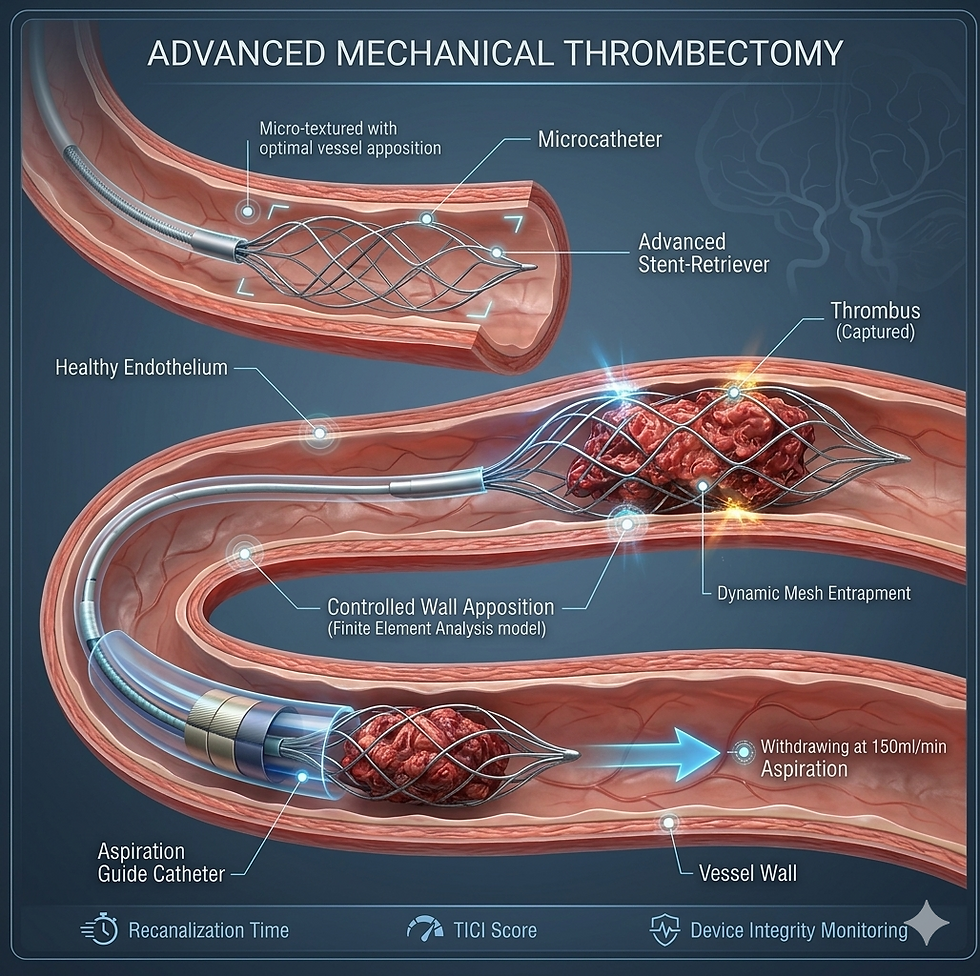
1. Treating Ischaemic Stroke (Blocked Artery)
Goal: Get the clot out. Fast.
Step 1: Access : A specialist inserts a tiny tube (catheter) into:
the groin (femoral artery) or the wrist (radial artery) to get access to the vasculature.
Step 2: Navigate to the brain. Using live X-ray imaging (fluoroscopy), they steer catheters up through the arteries until they reach the blocked vessel in the brain.
Step 3: They now have to remove the clot (blockage.)
And they have two main tools to do this: Stent retriever: grabs and pulls the clot out. Aspiration catheter: sucks the clot out
Often it’s a combo and this whole procedure is called mechanical thrombectomy. It’s basically like unclogging a drain - except you want to pull the clog out and not send it further into the brain. Unlike your sink - where the small drain tube connects to a bigger tube… so the clog can pass to the sewers… blood vessels in the brain get smaller and smaller. So pushing the clog down stream won’t work. The clot needs to be removed.
And thrombectomy can restore blood flow in minutes if done quickly.
2. Treating Aneurysms (Burst or Unruptured)
Goal: Seal the weak vessel so it can’t bleed - or stop the bleeding if it already has.
Step 1: Access and navigation
Same process: groin or wrist entry, then guide catheters to the aneurysm with fluoroscopy (X-ray guidance).
Step 2: Repair from the inside: Depending on the aneurysm, the IR team uses: Coils which are fine platinum coils packed into the aneurysm to seal it off. There are a range of materials also used today (Platinum, Platinum–tungsten alloy, Nitinol components, Hydrogel coatings, Polymer coatings, PGLA bioactive coatings, Stretch-resistant internal fibres.)
Flow diverters: A mesh stent placed across the aneurysm neck to redirect blood flow and let the aneurysm shrink over time.
Stents + balloons: Used to hold coils in place in wider-neck aneurysms.
For ruptured aneurysms
Same techniques - but way way faster, under more pressure, with neurosurgeons and neurocritical care teams on standby. (Note speed and specialist teams!)
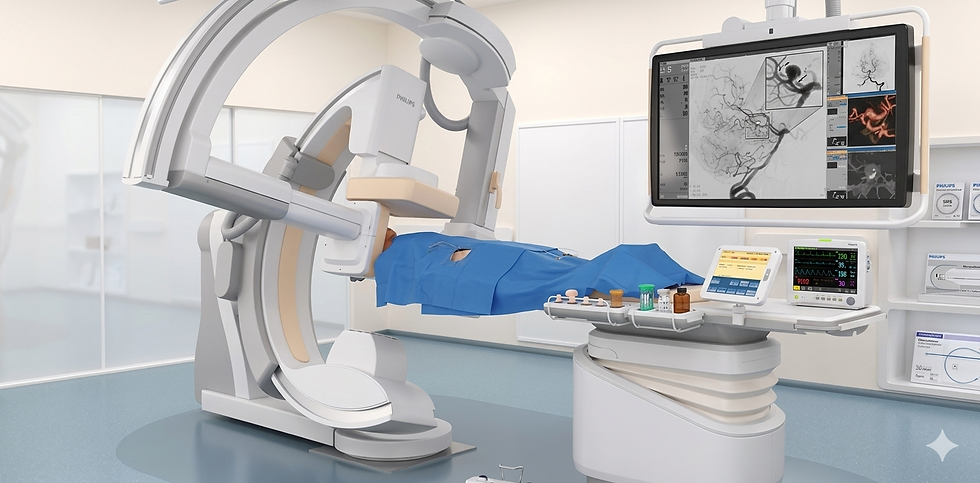
3. What the IR Lab Actually Looks Like in Practice
A large X-ray machine (biplane system for brain work)
A specialist at the table pushing guidewires millimetre by millimetre
Nurses managing meds and monitoring
Techs controlling imaging
The whole room focused on one thing: precision under time pressure
So to summarise: Whether it’s a stroke or an aneurysm, modern treatment is:
minimally invasive, catheter-based, image-guided,and entirely dependent on the skill of a highly trained neurointerventionalist.
So what’s the big elephant in the room?
The Massive Need: How Stroke and Aneurysm Care Fails Rural Patients Today
When someone in a rural area suffers a stroke or aneurysm, the biggest threat isn’t actually the clot or the bleeding - it’s distance. Geography becomes the real pathology. The care pathway is slow, fragmented, and fundamentally unequal compared to what an urban patient receives.
1. The Clock Starts Against the Patient
Remember for ischemic stroke, every minute costs roughly two million neurones.For aneurysm, every minute increases the risk of catastrophic re-bleeding.
(TIME is the enemy!)
Rural systems are built for stabilisation, not definitive neurovascular care. The gap is lethal in most cases.
2. The Ambulance Arrives… But Can’t Fix the Problem
Local EMTs (emergency medical teams) can deliver oxygen, basic neuro checks, and blood pressure management. But that starts to become the limit. They cannot perform thrombectomy, aneurysm coiling, or neurosurgical procedures. Which is what many patients require.
Their role is simple: stabilise and move as time leaks away.
3. The First Hospital Stop: Diagnosis Without Treatment
Most rural hospitals can run a CT scan to confirm stroke or bleed, but almost none have an interventional neuroradiologist set up. And this is where the problem starts.
They diagnose the problem but they can’t treat. So they immediately look for a larger centre to transfer to. Often, this alone burns 30–60 minutes. Million of neurones.
4. Transfers: The True Bottleneck
Here is where outcomes are won or lost.
The reality today in the USA:
The nearest comprehensive stroke centre may be 60–300 minutes away.
Air ambulances depend on weather, daylight, aircraft availability, and cost.
Ground ambulances are slow and often already stretched thin.
And every handover: EMT → rural hospital → air crew → destination centre — adds more delay.
The sad truth today is that most rural patients simply age out of the treatment window before they reach the specialist.
5. Arrival at a Specialist Centre
Only when the patient finally reaches a major urban or regional hospital does definitive care begin:
Ischemic stroke: mechanical thrombectomy.
Aneurysm: endovascular coiling or surgical clipping.
These centres are built around specialists who (by the way) are in very short supply and almost never based in rural locations. So your entering the realm of postcode (zip code) lottery.
6. Specialist Scarcity Makes Geography Destiny
There are fewer than a thousand interventional neuroradiologists across the US and even fewer across Europe. They generally cluster in large cities. So if you want to live through an event like this… relocate to a major city.
Rural hospitals therefore act as:
diagnostic stops
stabilisation points
and transfer hubs
…but (today) they are not normally treatment centres.
Whether a patient survives - or avoids lifelong disability - depends almost entirely on how close they live to a major hospital with the neurointerventional capabilities.
7. The Outcome: Rural Patients Are Statistically Disadvantaged
Because of delays, rural stroke and aneurysm patients face:
later treatment
higher disability
higher mortality
higher long-term care needs
In short:
A patient’s Postcode / Zip Code determines their prognosis. And in 2025 that is borderline outrageous.
Why This “Need” Matters
This is exactly the gap modern neuro-endovascular robotics and remote-capable systems aim to close. Rural hospitals diagnose stroke and aneurysm rapidly - they (frustratingly) just can’t treat them. Robotics, tele-operation, and magnetic navigation platforms are designed to turn those diagnostic islands into treatment-capable hubs.
The technology is catching up. The geography is not. And this has to be resolved - not just because of the clinical and societal devastation - but the cost of dealing with failed treatment is vast.
The Health Economics of Delay: Why Every Minute Costs the Country Money
When a stroke or aneurysm patient waits too long for treatment, it isn’t just their brain that pays for it. The economy does too. Delayed care converts what could have been a straightforward hospital stay into a lifelong expense… and the numbers are F’in staggering.
1. Delayed Treatment = More Disability
If blood flow isn’t restored quickly (stroke), or bleeding isn’t stopped fast (aneurysm), patients leave the hospital with far more neurological damage.
That means: more rehab, more specialist appointments, more long-term medication, higher carer dependence, more hospital readmissions, and often, permanent disability
Every additional hour of delay increases the chance a patient becomes a long-term cost rather than a short-term save.
2. The Lifetime Price Tag Is Enormous
The average U.S. ischaemic stroke patient generates roughly $140,000 in lifetime medical costs. That’s is just the average. Severe strokes, the ones caused by delays, cost society far more: full-time caregiving, disability payments, lost productivity, increased hospitalisations
A single severe stroke patient can easily run into hundreds of thousands of dollars in lifetime societal cost.
Aneurysms are even worse. Acute treatment alone can exceed $80,000, and long-term dependency regularly pushes the total into the low-six-figure range.
3. The Macro View: This actually drags on GDP
The U.S. currently spends around $100 billion a year on stroke when you include healthcare, rehab, lost work, and premature death. That's roughly 0.3% of U.S. GDP burned every year because the system can’t move fast enough. It’s ridiculous. But if we want to talk about areas where we can all move the healthcare needle - then it is right here.
Let’s not forget… a large portion of that cost comes from patients who: missed the thrombectomy window, arrived too late for coiling, had no access to specialists in their region, sat in ambulances or helicopters for hours…
These aren’t medical failures - they’re logistical failures.
4. A Small Speed Gain = A Huge Economic Win
If we could reduce disability by even 5–10% through faster access to intervention (robotics, remote operation, rural neuro hubs), the savings would be measured in billions per year. Let me say that again - BILLIONS per year. This is a cause worth fighting for.
Spread across a decade, you’re talking about tens of billions returned to the economy simply by treating patients fast enough to walk out of hospital instead of being carried out.
This is why there is such alignment of needs between patients - clinicians - hospitals - payers - society. You will not find a lot of resistance about fixing this issue.
5. The Simple Conclusion
Delayed stroke and aneurysm treatment isn’t just a clinical problem - it’s an economic tax.Every minute lost costs neurones, independence, and GDP.
This is the exact gap that neuro-endovascular robotics and remote interventional systems are built to close.
Hang on hangs on Steve… couldn’t we just train more neurovascular specialists instead of wasting time and money on robots?
Why We Can’t Solve the Stroke and Aneurysm Crisis With People Alone
This fair question keeps coming up: “Why don’t we just train more specialists and build more IR labs in rural areas?”Simple. Because the maths, the logistics, and the economics all say “no chance.”
Why?
1. You can’t actually mass-produce neurointerventionalists
Treating a stroke or aneurysm inside the brain’s tiny vessels isn’t something you learn on a weekend course.
A typical pathway: 4 years medical school, 5 years radiology, neurology, or neurosurgery, 1–2 years neurointerventional fellowship, 1–3 years of real-world learning curve in a high-volume centre: You’re looking at a decade-plus before someone is safely operating inside a cerebral artery. You simply cannot scale that workforce fast - or safely.
2. Rural areas don’t have enough cases to keep specialists competent
And this is a real issue. Case load drives competency - and this is why you need a hub and spoke network.
High skill = high volume.Rural hospitals don’t have volume. Most see 0–2 thrombectomies per month, and even fewer aneurysm cases. And that is not enough to justify the clinician full time. And they would not have enough cases to keep their skills up. A specialist in a low-volume area would lose their edge; and their accreditation. That’s unsafe for patients and unattractive for the doctor.
3. IR and neuro-IR labs are incredibly expensive
A single neuro biplane suite costs: $2.5–5M equipment; $1–2M construction; $3–5M per year staffing & support
It’s financial suicide for a rural hospital that may treat a handful of neurovascular cases per year to have a dedicated neuro IR suite. Even if you built it, it would sit unused most days.
(Hang on - I hear you say. But you still need that for a robot… right? Let me tackle that in a minute.)
4. Specialists won’t relocate to rural hospitals
Not because they’re selfish - because the system makes no sense for them. They need: surgical backup, anaesthesia support, a full IR team, consistent case flow, safe call schedules, academic advancement, stable family life
In reality: Rural settings offer none of that. You can’t bribe your way out of a structural mismatch. (You have to think about reality.)
5. 24/7 coverage is mathematically impossible
To run a safe neurovascular service around the clock, you need: 3–4 neurointerventionalists, specialised nurses, IR techs, radiographers, anaesthetists. Even if the hospital might see one case every couple of weeks… you still need all of this. No health system can afford that footprint in every rural town. It doesn’t add up - even with those devastating numbers.
6. Even if we trained more… they still cluster in cities
Let’s get real - doctors go where: the cases are, the teams are, the research is, the pay is, the infrastructure is, the schools and families are…
In reality what will happen - training more simply adds more to the same urban hubs. It doesn’t magically repopulate the countryside. People are people.
The Reality: You cannot fix the rural stroke/aneurysm problem by training more people, building more rooms, or hoping more specialists will move. The model doesn’t scale.
But robotics actually does: Robotic and remote neurovascular systems let one specialist cover several hospitals; rural hospitals treat locally; patients get thrombectomy or coiling without being moved; high-end skill can be delivered from anywhere.This isn’t a luxury…It’s potentially the only scalable solution the system has.
We talked a lot about the Interventional Neurologist and the 10 year pathway. So why is it so hard to do?
Come on Steve - even to use the robot you still need an IR suite and a team - this makes no sense?
People eventually come back to this argument : “If a Rural IR Lab + Team Is 90% of the Setup, Why Isn’t It Enough?”
Let me give my spin on this having worked across most of the world’s healthcare environments - and seen from massive urban to small rural set ups.
Unfortunately, because in neurovascular care, the missing 10% is actually the whole game.
Stroke and aneurysm treatment is not limited by beds, rooms, or nurses. It’s limited by one thing:
A specialist who knows how to safely navigate inside a brain artery the width of a piece of spaghetti. (I do live in Italy.)
You can have:
the room
the nurses
the imaging
the catheters
the monitors
the sterile field
the anaesthesia
…and still be completely unable to treat a stroke or aneurysm. Because the only thing that actually fixes the problem is the specialist’s hands. That’s the magic 10%. And without it, the other 90% is just expensive wallpaper. (Oooohhhh I can see you starting to understand where AI and autonomy may well come in later… hold that thought.)
Let me try and break it down and then come to the solution:
1. Almost every mid-size hospital already has the “90%”
Most rural/regional hospitals already have: cath labs, IR suites, fluoroscopy (not always bi plane as a note), trained IR nurses, radiographers, on-call general anaesthesia, emergency care protocols.
In other words:They already have the infrastructure for everything except the actual brain procedure.
So the room isn’t normally or in reality the limiting factor.
2. The missing specialist is the real bottleneck
You cannot run a stroke thrombectomy or aneurysm coiling unless: someone can navigate from femoral/radial access, up the aorta, into the carotids, into the intracranial vasculature, and manipulate microcatheters through tiny branches …all while avoiding perforation, dissection, and wire-induced injury.
That… right there.. is a decade of training condensed into a pair of hands. That’s the missing 10%. And it’s the hardest part of the entire system.
3. That 10% is the thing you cannot staff locally
Why?
Because rural hospitals: Don’t have the case volume, can’t justify the salary, can’t support the on-call burden, can’t maintain specialist competency, can’t attract the experts, can’t back them up with neurosurgeons or neuro ICU, Even if you built the perfect suite, that specialist will not move there.
This is why 90% isn’t enough.
4. Robotics turns that missing 10% into something scalable
Robotics makes the bottleneck portable.
The golden “hands” of the neurointerventionalist become: Remote
, sharable, scalable, deployable across many hospitals.
That final 10% - the part you cannot physically put into rural hospitals - becomes centralised and connected to all the other “90% sites” via telerobotics.
This is exactly why the economics suddenly work.
5. The simple bottom line
Rural hospitals already have the 90%. What they don’t have is the one person who can save a brain in the next 10–20 minutes. Robotics isn’t replacing that person.It’s letting them be everywhere at once.
That’s the difference between “almost enough” and “actually treating the stroke”.
Not convinced… you still need all the support team and more it’s not just the neurointernationalist you doughnut.
Okay - life is never cut n paste. But the gap between what they have today and being able to run remote stroke treatment and aneurism treatment robotically is not as far off as most may think. So what does a rural hospital actually need before installing a neurovascular robot (we’ve go to get to that yet.)
There’s a myth that you need a fully staffed, big-city stroke centre before you can use neuro-robotics.
I don’t think you do.
Instead here’s what I (and others) think a rural hospital really needs - and, importantly, what it doesn’t.
1. A Suitable Procedure Room (Most Already Have One)
You need one of the following:
A standard IR suite
A cath lab with decent fluoroscopy (for a few of the robots they are showing you don’t need bi plane.)
A small/medium biplane room if they already have one and the robot need biplane.
Not a huge, custom neuro suite.Not a full hybrid OR.Just a fluoroscopy room that can support a catheter-based procedure.
Most regional and rural hospitals already have this - and they are often sitting underutilised.
2. A Small Core Team (Already on Payroll)
You need:
1 IR/cath-lab nurse
1 radiographer/fluoro tech
1 circulating nurse
Procedural anaesthesia support (usually available in any hospital with an ER and OR)
All of this exists in even modest rural hospitals.
What you don’t need:
neurointerventional nurses
neuro IR techs
neurosurgeons
a dedicated neuro stroke team
Robotics removes the need for the specialist to be physically present.
(I won’t go into it here but already there are networks of tele supported teams happening today.)
3. Basic Upskilling (Weeks, Not Years)
Local staff need short, targeted training:
robot setup and shutdown
sterile field around the robotic arm
catheter and device loading
how to interface with the remote specialist
emergency protocols (already familiar from cath/IR work)
This is practical hands-on training - not neurovascular fellowship content.
Most staff say it’s actually easier than learning a new imaging system.
(Rural hospitals are not barns in a field.)
4. A Remote Specialist Hub (The Brainpower Lives Here)
This is where neurointerventionalists sit: centrally, with high case volume, backed by neurosurgery, backed by neuro ICU, backed by experienced teams.
One hub can cover multiple rural hospitals, 24/7, without destroying specialists’ quality of life.
This is the part that makes the entire model economically sane.
This needs to be a hub and spoke model.
5. A Transfer Pathway for Rare Surgical Cases
You need:
a transfer agreement with a neurosurgical centre
transport capacity (already used today for trauma, bleeds, TBI, etc.)
You don’t need on-site neurosurgeons for 99% of thrombectomy or coiling cases.That’s already how rural hospitals manage trauma and hemorrhages today.
6. Reliable Connectivity
Not fancy... just:
stable broadband or fibre
secure failover
a direct link to the remote operation hub
If the hospital is already transmitting CT scans to a stroke centre (most are), they’re halfway there.
7. What They Don’t Need (The Expensive Stuff)
No need for:
building a new fully equipped neuro-IR suite
hiring neurointerventionalists
staffing a 24/7 neuro rota
dedicated neuro ICU beds
surgical backup on-site
academic research infrastructure
This is what makes traditional expansion impossible - and in my mind robotics possible.
I believe… and you can argue against me…
Rural hospitals already have 80–90% of what’s required. Remote robotics delivers the missing 10% - the specialist’s hands - from a high-volume centre that can safely support it.
This could be the first truly scalable model of neurovascular care.
What a Robotic Rural Stroke Network Looks Like (My idea of a Future Map)
Take this for what it is. A medtech blogger just spit balling out some ideas of how this could look and work. And then I’ll get into the robots and how they could make this happen. Perhaps, we can imagine together a stroke and aneurysm system that actually scales.
This is not by building more mega-centres,. Not by trying to clone specialists everywhere.But by connecting the hospitals we already have into a single robotic network.
Here’s how it might work:
1. A Central Neuro Hub (The “Brain” of the Network)
This is a major stroke centre with:
neurointerventionalists
neurosurgeons
neuro ICU
high-volume workflow
round-the-clock capability
It basically becomes the control centre. Inside it, 3–5 neurointerventionalists can cover dozens of rural hospitals. They sit at robotic consoles just like pilots in an air traffic control tower - operating remote systems across an entire region.
2. A Ring of Rural Hospitals (The “Hands” of the Network)
Each rural or regional hospital has:
an IR/cath-lab room
a small, generalist team
a robotic endovascular system
basic anaesthesia
rapid CT capability
They no longer act as “diagnose and transfer” sites. They finally treat. Instead of patients going to the specialist, the specialist comes to them - digitally, in seconds.
3. When a Stroke Happens
The sequence becomes:
Patient arrives at rural hospital
CT confirms stroke
Remote neurointerventionalist logs in
Robot is prepped by local team
Thrombectomy begins within minutes, not hours
No helicopter. No multi-hour road transfer. No specialist sprinting across a city. Just treatment.
4. When an Aneurysm Bleeds
The same logic applies:
rapid CT
immediate remote review
robotic coiling or flow-diversion
if needed, transfer later for surgical care
Crucially: bleeding is stopped fast, not two hours later when the patient finally reaches the big-city centre.
5. The Staffing Model
This is where the economics finally make sense.
At the hub:
3–5 neurointerventionalists
24/7 availability
built-in surgical backup
At each rural site:
2–3 IR/cath-lab nurses
1 radiographer
anaesthesia support
A single hub specialist can treat:
Hospital A at 09:15
Hospital B at 10:00
Hospital C at 14:30
Three different towns. Zero travel. Zero downtime. The first scalable neuro workforce model in history??
6. Connectivity as the Backbone
From everything I’ve seen so far I don’t believe you need exotic infrastructure. In fact if this becomes a requirement I think we have more friction to make this happen. But if something better is needed - then there are companies that are looking at this like Sovato.But so far I think you just need:
hospital-grade broadband
simple failover (back up connection if the line goes down.)
secure remote-control protocols
Many stroke networks already transfer CT scans and run telestroke consults - this is the natural next step.
7. Outcomes Change Dramatically
Today:Rural stroke → long delay → disability or death.
With a robotic network:Rural stroke → treat immediately → walk out.
This shifts: Mortality, disability, rehab burden ,cost to the healthcare system, cost to GDP.
It’s the first model that doesn’t collapse under workforce shortages.
8. The National Map
Imagine this:
1 hub per 3–5 million population
8–15 robotic hospitals per hub
Coverage for millions with a specialist team that never leaves the building which mirrors: air traffic control / Telestroke / military drone operation / remote surgical telepresence.
…It’s the same principal just applied to saving brains instead of flying aircraft.
My simplistic vision…
Robotics turns every rural hospital into a mini neurovascular centre. The expertise stays centralised. The treatment becomes local. The network becomes scalable.
For the first time, geography stops predicting who gets to live or walk again.
Telerobotics is more about local networks than transatlantic demos
Having spoken with several teams in this area - they feel that the whole “telerobotics” thing is a little distorted in neurovascular. So let me try to redress the balance a little here.
Can a telerobotic stroke thrombectomy be done technically across a 5G network across the Atlantic - well yes. And that has been demonstrated just recently. So are we going to be having aneurisms coiled at 15,000km distance every day… probably not.
I think the tech demo of large distance telerobotics in neuro is cool, and shows the systems can do it. What is shows is that if you can do it at 15,000 KM you can probably do it at 300 KM just as well. (That works in miles as well for my US colleagues and British compatriots.)
My view is that the reality is the hub and spoke regional network as described above. It will be about hospital systems within their own network - with their own operating rights and paperwork and payments - using this capability to cut the distance and time within their regions. It is slightly different than maybe some of the other tele surgical uses. Of course proctoring - tele preceptoring - demo cases and even the odd super difficult case “could” be done - but I think (and so do many others) that the day to day use of this is in the hub and spoke of the regional hospitals. and that is where the biggest value gains will be.
Why Being an Interventional Neurologist Is Hard. And How AI and data could Help
One of the key things about putting a robot between the patient and the caregiver - data.
Let me start by something that has been said about da Vinci time and time again. Besides the precision you get - the fact you have a computer between the caregiver and the patient should never be underestimated. The data (both ways) that streams through the system is part of the secret sauce of the future of medicine. The data analytics and insights are foundational today for robotic systems - and the data lake generated is critical in training the emerging AI systems.
Forget telerobotics for now and zoom in on “Why put a neuro robot between the patient and the care giver today?”. Data.
We can start to collect masses of data and create local feedback loops within the same IR room. You don’t need to be 300 Km away to get the benefit of the precision and the data. This will be critical in neuro - with accurate and precise catheter advances - force feedback - image guided navigation and insights others can learn from (including self improvement of the neurologists.)The robot in itself - local will bring immense value. Why?
Interventional neurology isn’t just another subspecialty. It’s one of the hardest technical skillsets in medicine. You’re navigating wires and catheters through arteries the width of a coffee stirrer, all the way from the groin or wrist into the brain. One wrong move and you can dissect a vessel, rupture an aneurysm, or worsen a stroke. It takes over a decade of training to safely (and proficiently) guide a microcatheter into a cerebral branch measured in fractions of a millimetre.
The problem? Skills don’t just require intelligence - they require volume. These specialists need a steady stream of cases every week to stay sharp. That’s why they cluster in big centres and why rural areas can’t keep them: the caseload simply isn’t high enough to maintain proficiency.
And you are doing all this while on the fly interpreting radiology images - not easy.Biplane imaging looks simple from the outside: two X-ray views of the brain’s arteries taken at the same time, one from the front and one from the side. But to an interventional specialist, it’s like reading two maps of a city you’ve never visited, in two different languages, while driving through it at full speed.
You’re not just looking at the images - you’re mentally reconstructing a 3D vascular maze in real time. Something AI is actually very very good at BTW.
Every branch, every curve, every narrowing matters. A vessel isn’t a straight pipe; it’s a twisting river system. Tortuosity - those S-shapes and 90-degree bends - turns catheter navigation into a high-skill art. One vessel may loop like a corkscrew, another may narrow down to a thread, and another might take a sharp turn behind the jawline. The biplane system flattens all that complexity into two projections. The experts brain has to fill in the missing dimension.
This is where the difficulty goes up. A smooth curve in one view might actually be a dangerous kink in the other. A vessel that looks open on the lateral plane may be nearly occluded on the AP plane. A subtle narrowing may disappear entirely in one projection and only reveal itself in the other.
The neurologist has seconds, not minutes, to interpret this, decide on a safe path, and steer a microcatheter that’s thinner than a human hair through a vascular network that punishes even small errors.
This mental load is why the training curve is long and unforgiving. It’s not enough to understand anatomy; you need the ability to translate two flat images into a living, shifting 3D environment and navigate it with millimetric precision.
And it’s exactly here that robotics and future AI will be game-changing: stabilising motion, assisting interpretation, predicting vessel geometry, and reducing the cognitive burden so more specialists - and eventually more hospitals - can safely treat the patients who need them. Not at distance but in local usage.
In my mind AI combined with robotics isn’t going to replace the specialist, but it can support them: analysing images instantly, predicting vessel paths, flagging risky anatomy, stabilising robotic movement, recommending device sizes, and eventually assisting in real-time navigation. Instead of one expert having to rely purely on human judgement and muscle memory, AI and data will provide a second set of superhuman eyes and hands. All delivered by the robot - at distance.
The result? Specialists become faster, safer, and scalable. And the expertise that once lived in a few major hospitals could be extended across entire regions. Just when the field hits its workforce limit, AI and robotics becomes the force multiplier it desperately needs.
But to do that - you need to start local and then move to the telesurgical version of the system. Locally using a robot will bring a vast set of advantages and up everyone’s game - just as da Vinci did in surgery. Let’s not forget 18 million cases have been done locally - not tele surgically and the benefits have been shown.
I’m trying to say - don’t get over hung up on the telerobotics today - in your mind just start to think local robot and what da Vinci did for surgery. It’s slightly different but a lot of parallels.
Issues in the robotic market place today and why you should pay attention to neurovascular robots
For any of you following the whole health robotics space and where it is going - there are some major shifts happening - and 2025 has been full of them. But one I want to talk about is with relation to the world of Da Vinci style laparoscopic robots. I’ll explain it in one work - “Saturated.”
There are 36 systems out or about to be out in that space and finding room there is getting harder. My recent commercial workshop focused on finding a Unique Proposition or die trying. For investors - analysts - industry watchers and industry operational folk. Today is about looking beyond the saturating market of lap robotics and surgical robotics and seeing where new technologies are heading.
Now a disclaimer. A lot of what I’m about to talk about is not “new” per se. Some of these companies have been at this for a decade. But one thing you need to understand is that making long flexible robots is hard - making them steerable and controllable to sub millimetre accuracy - is very hard (especially at distance). So many of these systems have been baking a long time. So why now? I’m talking about this now as we are entering into more and more regulatory clearances and clinical cases. It’s becoming real. Plus the technology (AI Nvidia) and the telerobotics (5G networks etc) have all come together now - in a confluence moment.
So we all need to look beyond the classical surgical robotics and into the next frontiers of health robotics.
Flexible robotics and their challenges
I am super fortunate to spend time with some of the utter master engineers behind many robotic systems - and a few that have worked on most of the emerging systems. One thing they always say to me is that going from rigid robotics to flexible robotics is a whole other challenge.
Now let’s start by just talking about the challenges of flexible robotics in the GI space. How you get the robot to navigate and have the tip yaw and pitch - is difficult in itself. And then to have all of that control work (won’t go into details here as why length becomes an issue - maybe for another day) and have stability and precision - ability to push and pull and twist (torque) to get these flexible robots around the bends. None of it is easy. “The control software is a pig” as was said to me.
So if this is a major challenge for a large flexible GI robot (up to 10mm diameter) - it gets harder as you go to say… a bronchial robot at 2-3mm - trying to pack all those control wires into the wall and still have enough lumen left inside to be useful. Plus have things like fibre optic shape sensing technology built in.
Now drop down that size again to - PCI catheters and Neurovascular catheters at 1-3mm and the challenges go up exponentially - and now we drop again to neurovascular micro catheters - <1mm to 2mm. It starts getting unfathomable how small these things get and somehow we want to control them over nearly 2 meters and allow them to drive around incredibly tortuous bends. Having enough wall strength to push and pull and drive them where they need to go.
One of the secrets of course that with most small catheters - to allow them to torque (twist) - push and pull - they basically run over a “rail” otherwise known as a guidewire. These small wires can run the length of the vessel - get around all the corners and act as…. Well a guide for the catheter to run over. This is part of the magic of how interventionists are able to get to were they want to go - traverse blockages and narrowing and get around tight bends - through junctions and deep into the brain. It takes vast skill to be able to get that tip of a guide wire to go where you want it to go - at speed - and without causing damage - all by looking at an imaging screen.
Guidewires are a critical part of this puzzle - as someone that did a lot of work in cardiology - I learned pretty quickly that guide wires are a science all to it’s own - go here - this will help as these things are not what you think !
But in essence - you have a long wire - and if you form a curve at the tip you can rotate the wire to have the bend be to the left - to the right - up or down. (Anywhere in between). So if you come to a bend or a junction you can control which way the tip points and as you advance follow that direction. (Sorry that sounds so basic but I need to keep this simple today.)
Once you get the guidwirie where you want it - say to an aneurism - you can then slide over it a catheter which will rail its way to the same location. And there you could deliver a coil or other device.
Again… getting that guide wire where you want it sounds simple in my blog - but it is hard. That torquing and pushing and pulling and wiggling is also fraught with danger - perforations - dissections and more.
Why am I talking about this when talking about flexible robots?
Because more and more “steerable” devices are coming - steerable catheters - that use either concentric tubes, wires or hydraulics inside to move the catheter tip left and right and up and down. So as you advance you can literally steer to the area you want to go to.
And well robots are very good at steering things. It removes a lot of the complexity - and can even make sure that the operator is not having to hold the catheters and advance - whilst siting next to 2 X-ray machines (ya get it!)
The robot driving either the guide wire, the catheter or the device keeps the operator away from radiation, has greater precision (theoretically) can potentially torque things more accurately or even control the direction of a steerable catheter.
And this is where we enter the realm of endovascular robotics…
Endovascular robots - let me set the scene
This in itself is a massive category - with sub categories (neurovascular being one.)
But there are peripheral vascular robots, peripheral vascular access robots, and cardiac robots - such as coronary artery robots and endo cardiac robots. All of these are long catheter based robots that drive inside vessels to get where they need to go.
A neurovascular robot heads north to the brain. Up through the arteries - past the carotids and then to smaller and smaller arteries in the brain.
All endovascular robots face the same challenge. They need to control long thin catheters (well some) inside tortuous blood vessels - full of blood - with very delicate small movements and under fluoroscopy (X ray) sometimes with CTA (computer Tomography Angiography or IVUS (Intra vascular Ultrasound.) But it’s not the white light optical imaging we use in laparoscopy or bronchoscopy today. (Well not yet but that’s another story.)
But not all endovascular robots try to fix the navigation problem in the same way. And this is where we get to the most interesting part and why there are so many companies with so many approaches.
So we could tackle the issue of navigation in a few ways.
Make getting guidewire to where it needs to go easier and faster
Could make a more steerable guidewire
Could skip the guidewire steering and go with steerable catheters
Shape sensing catheters that segmental follow the curvature of the vessels.
Etc
Back to point 1, we have a few approaches to how we could get that guidewire there. We could have a steerable guidewire where it is steered from the “use end” or proximal end. Or we could drag the guidewire by the distal end - and we could drag it with magnets - clever magnets of course.
All of these have pros and cons - and all of the following companies are using different methods to try and get that robotic navigation of the guidewire or catheter to the lesion as fast as possible, as atraumatically as possible, as reproducible as possible and with the user having the most “acceptable experience” to get it there.
Oh yes we will dig into Haptics - as much of this today is about “feel” and “touch” and a big debate is “Do we still need haptics?”
Seems to be a theme in robotics. But after that very long introduction I hope now the insights into the following companies will make more sense.
Neurovascular Robotic Companies - it’s complex
Okay I’m going to put my hand up here and make sure I’m clear - before we go into this. Many of the capabilities of the neurovascular robots are sort of the same (in very rough terms) as cardiovascular robotics and peripheral vascular robotics. Guidewires - catheters - microcatheters - tool exchanges - inside vessels - blood - navigation - tortuosities - and on and on.
But there are subtle difference - where Peripheral vascular tools and Neurovascular tools share things like over the wire exchange of tools (so the guidewire goes all the way through device) vs in Cardiac where they use a Rapid Exchange system (guidewire inter the tip of the device and exits a little way back from the tip through a side channel.) This affects rapidity of exchange - simplicity of exchange but also the stiffness and pushability - torquability etc etc etc - (guidewires are not just dumb bits of wire.)
Why am I starting here - because some of the companies below are super focused only on Neuro as a start - where as others are going via routes like peripheral - or cardiovascular before they go to neuro.
And this is important as there seems to be two schools of thinking at the moment out there. One is that the robots for PV and CV have been out a long time and shown little to no real “benefit” - and Corindus in cardiovascular is held up to my face time and time again. And Sterotaxis is another that is held up again and again as “great idea but no one really wants it.”
as I often say: Life is about timing. And when I look at this, I see this has been an issue of coming together of a confluence of technologies. (I’m going to butcher this - but it is so clear in my head…)
Corindus people, shout me down if I’ve got this wrong. This is my opinion. Corindus (by the way lots in names as you will see later) went for the heart. They were all about making getting guidewires into the heart easier through robotics. But honestly - if you ask most interventional cardiologists - except for some very complex vessels - most cardiologists are capable to rapidly get the guide wires where they need to go; and then do the procedures they need to do. The robotic guidance of the guide wire didn’t really help them or (importantly). Hangs patient outcomes enough. But the theory was the user could take off the heavy lead apron - get away from the X-ray and control the robot from behind a shielded cockpit.
So in the mind of many buyers, the main benefit was for the Interventional Cardiologist - in reducing X-ray exposure. Now I’m going to be brutal. Patients didn’t really do better - so hospital management didn’t really care (sorry) about if the user got less exposure to X-Ray. I mean they have lead aprons to protect them right? The management didn’t seem to really care if sitting rather than standing with lead was better for the interventionists back. And anyway - they got the guidewire there - but the still had to come back top the table to do more parts of the procedure. So was there a big enough advantage to justify that spend?
Basically the benefit to the user was seen as “so so” and most importantly the benefit to the patient was felt as negligible. And when you try and convince hospitals to get an “expensive robot” the equation didn’t stack up. So we saw a very limited uptake - and when Siemens got the system they all but abandoned the cardiac push. Okay this is how I think it went down based on everything I’ve read, seen and had from 1st hand people selling the system.
You have to also look at this whole segment and understand that many of these companies are well over a decade into their journey and they are now pivoting from PV and CV (or changing messaging) now - because a few things have changed.
I talked earlier about the confluence of a few things - Data - AI - Telerobotics. And it is these things that, in my mind really, change the dynamics in PV, CV and especially NV: and make the “Why Now.” And these same reasons are why PV and CV might suddenly make a resurgence if it is also combined with NV?
In fact several of the following companies seem to be banking on it.
One insight I got was about the regional hub and spoke model. I strongly believe that the regional experts - flying robots remotely in PCI labs in the rural areas is the massive win for NV robots. But you still need real world use that makes total usage sense. That is about “how much will the robot be used?” To keep proficiency up along side how much will it cost.
You see - as I’ve said for years - robot capital costs is simply related to usage. More usage - more the capital costs come down. Using a complex expensive robot 1 or 2 times a week with different teams just during emergencies will not, and cannot, be that economical. But it also caries the risk that if it is just pulled out for those time sensitive and super complex NV cases - the teams are only getting knowledge usage when they are in the hot situation. not the best time to be getting used to a system.
What would be more ideal is if the local team is also using the robot day in day out for PCI or peripheral vascular cases. Which are often already done in many of these centres (not every but…)
If the local team could use the local system (not telerobotically) on a more frequent daily basis - then when the hot NV case comes in - it’s just part of routine.
If it is also being used routinely it is leveraging the fixed costs way better - and of course helping users get less radiation. But that might only work if the robot does not have expensive - extra big costs tied to it’s standard daily usage. Yes there is margin in these procedures - but part of the whole complex argument will be about which razor blades can you use with the razor. Interventionists are often very very choosey on what products they use - leading to a wide choice of product and specific tools for specific jobs. And this all starts to tie into the overall economics of the robot. Is it a capital purchase - lease model - razor / razor blade model?
To make any of these models work, a basic philosophy will need to be - can we use the (expensive) tele robotic neurovascular robot for day to day care as well? Can we use devices off the shelf? Can we use it locally and get any actual benefits? Will the economics stack up for the hospital and the company?
Stand alone 1 or 2 emergency cases a week may struggle to make the usage and economic models work… I think it will need to be used daily for CV and or PV cases to make real logistical and economic sense.
Local benefits are reduced radiation (and if you can do more than just guidewire manipulation get away from the X-ray for longer.) Data - and that is becoming critical for insights for users. Plus you start to get data to train AI for future assistive uses. And teams get regular usage.
Telerobotic benefits - we have talked about adnausium above.
So is to the confluence of Telerobotics, AI, DATA and of course minimising radiation (This is gaining momentum) that makes NOW the logical time to get the hub and spoke model for tele robotic neurovascular - but also is it the logical time for the local uses in PV and CV?
Let’s have a look at what different companies are doing and then I’ll come back with some thoughts.
Alphabetic order of endovascular robotics companies:
NOTE - much of this what I can find summarising web searches - AI LLMs - but also in many cases talking to the companies. It’s for general overview only. Don’t hold me to it and for secrecy reasons I cannot divulge everything I know.
I want to thank Dwight Meglan for his contribution to the list of systems here - many were off my radar.
Artedrone
“Arterial Drone” - may give a clue in the name.

Artedrone is a Paris-based Truffle Capital portfolio company, founded in 2017, developing SASHA, an autonomous microrobotic system for mechanical thrombectomy in acute ischaemic stroke.
They claim their aim is to “democratise” stroke intervention by allowing cardiologists and radiologists in non-neuro centres to perform thrombectomy.
The SASHA concept uses CT/MRI to create a digital twin of the patient’s cerebral vasculature and pre-plan a route to the clot; a catheter is advanced to the carotid “base camp,” after which a magnetically guided microrobot, carried by blood flow and steered by external magnetic fields. Think like a mini parachute being dragged along by the blood - with the magnetic arm helping it decide to go left or right.
They claim it autonomously navigates distal cerebral vessels, attaches to the clot via a magnetic suction-cup mechanism, confirms grip in a feedback loop, and then retracts the clot through the catheter for removal.
In April 2025 the company announced that SASHA had successfully performed end-to-end autonomous thrombectomy in multiple preclinical models, including in vitro human vascular phantoms and in vivo porcine cerebral vasculature with both analogue and native clots.
The results were submitted for peer-review.
Led by CEO Liane Teplitsky, formerly head of Zimmer Biomet’s robotics programme,
For investors “Artedrone is currently seeking around €20 million in Series B funding to complete preclinical validation and is targeting first-in-human studies around 2027” Can’t confirm but maybe Liane can comment.
They are positioning SASHA as the first fully autonomous neurovascular robotic solution specifically designed to expand access to thrombectomy beyond specialised stroke centres.search
Flux Robotics

Flux Robotics is a Dutch vascular-robotics startup spun out of the University of Twente, developing a magnetic-navigation system that steers magnetically responsive guidewires inside arteries to speed up and simplify complex endovascular procedures.
Their platform, Flux One (and the upcoming Flux 2), uses an electromagnetic coil mounted on a robotic arm to generate precise magnetic fields that guide the wire through tortuous or occluded vessels without the torque, push–pull, or radiation exposure that slow traditional manual techniques.

Early phantom and preclinical data show faster navigation, improved accuracy, and the potential to make challenging interventions like chronic total occlusion crossing or peripheral arterial disease treatment more reproducible and accessible, particularly in centres without specialist vascular operators. Still pre-commercial, Flux recently secured new investment to advance toward first-in-human studies, positioning itself as one of the more promising entrants in the next wave of vascular robotics.
Okay so they are a peripheral vascular company - and they seem pretty focused on peripheral; but there is no reason that this system cannot be used to get guide wires for PCI or intracranial vessels. This is where I think that some of these robots will span the continuum of endovascular care. I can’t say for sure they will go to Neuro - but it is the path of quite a few below, and would not be impossible for them to head north.
Imperative care

I’ve been pleasantly surprised by how much fan loyalty there is is for Imperative Care out there. People think they are doing amazing things in stroke care.
They are a California-based stroke company focused on building a vertically integrated, next-generation neurovascular platform rather than a single device, centred around its Zoom stroke system.
It’s a high-efficiency aspiration thrombectomy, advanced access catheters, and complementary technologies acquired through its subsidiaries (like Truvic for peripheral thrombectomy and Kandu for tech-enabled rehab). Their strategy is to own the entire stroke pathway - from rapid clot removal to post-stroke recovery; using purpose-built aspiration catheters, large-bore access systems, and data-driven rehabilitation tools to improve outcomes across all phases of care.
They have been developing the TELOS platform.
Telos is the “in-development: robotic/automation platform from Imperative Care, organized under business unit Telos Health which now redirects back into Imperative Care. So they seem to have come out and then gone back in.
Their stated mission behind Telos: to make endovascular clot-removal (thrombectomy) more accessible and standardized by combining robotics/automation with established clot-removal technology. Extending reach beyond high-end neurointerventional centers.
What Telos is supposed to do:
The platform is being built to enable aspiration-thrombectomy procedures (for ischaemic stroke) under robotic assistance; not just on-site, but with remote-capable (telesurgery) potential.
Telos aims to integrate with digital/remote operating-room infrastructure: in 2025. Of note is that Imperative Care announced a partnership with Proximie (Hi Nadine) (an OR-digitization / telesurgery software vendor) so that video, audio and telemetry data during thrombectomy can be shared with remote physicians via a Telos-specific “version” of the Proximie platform.

The vision emphasises making stroke treatment geographically agnostic, i.e. making mechanical thrombectomy available even in centres that lack experienced neurointerventionalists; by using robotic automation (What I was saying above.)
Telos is not yet commercially available, nor approved, and the platform remains in development.
Imperative labels Telos as “a future-oriented robotic platform.” The publicly stated goal is to drive innovation that expands access to life-saving stroke and vascular thrombectomy.
Business wire said “If successful, Telos could substantially increase access to mechanical thrombectomy - potentially reducing stroke morbidity by making timely treatment available even in centers without neurointerventional experts, or via remote operators.”
“This is important given the existing care gap: as many stroke patients don’t receive thrombectomy today.”
My observation is that by combining robotics & remote-capable orchestration via Proximie; it’s clear there’s a push toward “tele-stroke robotics.”
Hansen Magellan (sunset)
Honourable mention… but important speculation.

Hansen was one of the earliest pioneers of intravascular robotics. Its Sensei and Magellan systems demonstrated that remote-controlled catheter navigation, precise distal tip steering, and reduced operator radiation exposure were technically feasible and clinically usable. But their business model of expensive, dedicated robotic catheters, high installation and running costs, and limited therapeutic flexibility, I think, ultimately proved commercially non viable. Their acquisition and exit teach us all a key lesson: robotic platforms must balance technical sophistication with economic scalability and compatibility with a broad set of devices to survive long term. And I do think this is where - if you can use it for NV, PV, CV - the economics might stack up.
Why have I raised them here. Because (although grey and hard to find exactly) if you look that Fred Moll was behind Hansen (now in th X Cath video you should note that well) - and that wrapped into his Auris company - which then got acquired by JNJ. Hmm what Ottava? NO!Many don’t know but JNJ has a neurovascuylar division… Cerenovus.(https://www.jnjmedtech.com/en-US/company/cerenovus/all-products) .
So technically all the patents for Hansen (and a lot of the know how) are inside JNJ. And it has not been lost on me that they are strongly into cardiac at the minute and cather based cardiac for PFA and Shockwave. Plus they have Monarch - which in my mind is all linked. And as noted above, they rebranded their Codman business some time ago as Cerenovus. Now call me a conspiracy theorist but… I could imagine there are discussions within about how they could robotise their cardiac and neuro business using the old Hansen technology - and how they could lead them way more towards neurovascular robotics. (All Speculation but with some foundation.)
So I thought it was just worth a mention. Especially as this is in the bucket of steerable catheter systems and the IP for Hansen was early and strong.
Magnendo

Magnendo is a Cambridge, MA–based neurovascular robotics startup (founded around 2024) spinning out of a research line at MIT. They are building a magnetic-steering, soft-robotic guidewire platform designed to navigate the tortuous cerebral vasculature for stroke and aneurysm therapy.
Their technology embeds magnetic particles into a flexible guidewire tip and uses an external robot-arm magnet + magnetic navigation to steer through brain arteries. This potentially enables access to distal or complex vessels that conventional guidewires struggle with. Possibly reducing risk of vessel perforation or dissection and shortening procedure times.
In early 2025 they secured pre-seed funding from investors including Kakao Ventures and Base Ventures to advance platform development and collaborations with medical centres.
Of note there are some well known robotics experts on board including Miki Rosenberg former Medtronic robotics division. So they have a lot of know how to do this.
As of now Magnendo remains pre-clinical / pre-regulatory. From what I can see the system is not yet commercially available, but it represents a promising next-gen neurovascular robotics effort aimed at expanding safe, accessible stroke and aneurysm care.
Microbot Medical
I’m gonna start with a personal note from my friend and CEO Harel Gadot - CEO and Chairman. He says it the best about this space - “It’s a marathon and not a sprint.” - Damned right!!
I can remember when he and his team were first discussing totally disposable robots that you could hold in your hand.

At that time many people said “Has Harel gone mad?” But between then and now you would be amazed how technology has allowed more and more robotic systems in many specialties (such as vascular access - Intubation - needle delivered therapies and more) to become small hand held robots. Maybe this is not so crazy after all?
Microbot Medical (NASDAQ: MBOT) is a med-tech company that has just launched the first commercially cleared version of its LIBERTY Endovascular Robotic System. It's a single-use, remotely-operated robotic platform designed to deliver and manipulate catheters/guidewires for endovascular procedures (initially peripheral vascular, but with neuro and broader vascular applications in scope). Critically, they got FDA 510(k) clearance Sept 2025.
After years of preclinical work (100+ catheterisations in phantom/animal models with a ~95 % success rate and no intraoperative complications) Microbot is shifting from development into commercialisation:
Some big recent News: Emory University Hospital have already adopted LIBERTY, and a limited US launch began Q4 2025 with broader rollout planned for 2026.
Beyond human-driven procedures, Microbot is exploring “robotic telesurgery” collaborations, e.g. a partnership with Corewell Health in 2025 to assess remote interventional procedures using LIBERTY.
The company has also strengthened its IP: in August 2025 it secured a patent covering a modular robotic surgical system architecture that should help expand LIBERTY's adaptability across anatomy and procedures.
Bottom line: Microbot is now one of the first (Actually I think the first and only) company to attempt scaling vascular (and potentially neurovascular) robotics by combining disposability, catheter compatibility, remote navigation and a go-to-market push.
Why I want to draw attention here - and again take all of this with a pinch of salt as I’m just imagining here. But what happens when you get a disposable hand sized - remote robot?
The first paradigm that changes is “set up.” Tap it - unwrap it - connect it and use it. Then throw it.
“Disposable robot? Are you insane?” - yes and no. Many of these interventions are time critical - and ripping open a ready to go system that requires little to no set up makes the world of sense in time critical events. It also starts to make sense for “training.” Remember we talked about remote rural centres - and well the less assembly a team needs to do - the faster they get to proficiency. In my mind a huge part of design ethos (and Intuitive know it by the way) is efficiency in procedures - and although disposables are often criticised for costs - in these cases that efficiency pays back 100X.
I’m going to have one final fantasy here - as I’ve seen some new imaging modalities in the works - and I’m going to go super far fetched about crushing the time down to remove thrombus. Imagine that the in field Emergency team has this like a defibrillator in a pack ready to open. They gain peripheral access. In the ambulance is a new modality compact imaging system. The robot is ripped open - a trained medic gets femoral access - sets up the robot - which is connected to the regional medical hub via a 5G link. The throbectomy is done remote while the patient is in transport ready immediately run to the rural hospital.Fantasy? Yes maybe today. But it would take systems like this to really change the game. (Sorry I digress.)
Nanoflex
I remember a discussion with the CEO Matt Curran at the time they were spinning this technology out of ETH Zurich. I thought it was super interesting but was so deep into surgical lap robotics I couldn’t quite see the “why.” To Matt’s credit he was all in - able to see forwards to today. I think he made a smart decision.
Some background from their site:
“Founded in 2021, Nanoflex Robotics was spun out of a leading research university in Switzerland, ETH Zurich. Today, we are a medical device company specializing in the development of telerobotic solutions to treat a range of critical endovascular diseases. We are driven by our mission to widen access to lifesaving treatments and seek like-minded partners, hospitals and physicians to join us on our journey."
Now note well - it is a range of critical endovascular procedures - not just neurovascular. As I said earlier the pathway to the brain may be via the PV and CV routes first - slightly easier regulatory pathways and maybe slightly easier technically. But this starts to fall into the category of - remote robot that can be used in PCI, PV interventions and Neuro.
Does it follow that model of “value as a local robot for local needs” - telerobotically capable for when the high stakes neurovascular cases arrive?

It’s another magnetically driven system - but unlike others where the magnets are waved around on robotic arms - they have a static magnetic system that alters the 3D magnetic fields inside to give directionality to steer the “Ultra flexible magnetic devices.” Note they do not say “just guide wires” on their site. Using imaging and mapping they allow a user to drive the catheter around the vessels.
Like many of the system it is not just about “driving and guidance” it is about speed - and potentially reduced trauma. And of course - telerobotic.
From their site : “Safeguarded as a trade secret, our AI-compatible software enables secure, remote connectivity for endovascular interventions, regardless of geographical barriers. Telerobotic interventions offer patients more treatment options, while reducing physicians' exposure to harmful x-rays”
And to prove that (like many on this distinguished list) they are doing remote transatlantic studies - https://nanoflexrobotics.com/nanoflex-robotics-conducts-first-transatlantic-remote-animal-thrombectomy-study/
But again from me - I think these are great long distance demos - but they are tech demos to show stability - safety of the system. And if you can do at long distance… you can do at short distance. Such as in regional hubs.
Navigantis

I had the pleasure to recently speak to the team at Navigantis; and love their approach and enthusiasm. We talked a lot about the philosophy of the entire space. Here’s some background:
Navigantis is a Miami-based neurovascular robotics startup developing VASCO, a catheter-navigation robot built for diagnostic cerebral angiography, tumour embolisation, and ultimately mechanical thrombectomy. The company raised a solid Series A to push the platform into trials, and has already completed its first real clinical neurovascular cases, putting it ahead of most early-stage competitors. Yes they have done cases !
“VASCO is still investigational, but Navigantis is positioning it as a practical, workhorse neuro-robot aimed at everyday endovascular workflows rather than moonshot autonomy - with a long-term plan to enable remote stroke intervention once the core system is fully proven.”
A lot of what they are doing is still in stealth and I will keep it in stealth. But they did have strong opinions that the robot needs to bring value to the local users not just telerobotically. Data - AI and then how telerobotics is a regional game changer within networks not a global showcase.
It’s clear that the trifector of Data - AI - Telerobotics is high on their list - and it feels a very rational approach. Build value and experience for local use first.
Remedy Robotics
Still in relative stealth mode - let me read a couple of clues from their website:
Now note this first statement - “Flawless, immediate cardiovascular intervention for every patient, everywhere.”

The are focused here on cardiovascular. But as I’ve said - many of these systems can be adapted to do CV, PV and NV. I cannot imagine that after the kerfuffle around Corindus - Pivot will not have been a key phrase at any board meeting and advisor meeting.
In fact - just below the BIG statement is “Stroke, heart attack and other cardiovascular diseases kill and disable more people than all cancers combined. Endovascular intervention is the gold-standard treatment for cardiovascular disease, yet tragically most patients cannot get to a specialist center that offers it before it is too late.” - with Stroke leading the paragraph. Words are important.
“Where We Have Come From
“In early 2022, our co-founders David Bell and Jake Sganga bought a second-hand X-ray and lined a Venice Beach garage with lead. Not long after, Gregory Kahn – now our head of machine learning – dialled in from Berkeley to remotely drive our first prototype robot. Since then, we’ve assembled an elite team and built an incredible product with input from clinicians from around the globe.”
So let’s first note that machine learning (AKA AI) features heavily on their minds. And the fact they also discuss telerobotics is clearly important.
They continue: “Throughout this time, our mission has been unwavering: deliver flawless, complication-free endovascular intervention to every person on the planet be they in Kinshasa, Alice Springs, or Alaska.”This in my mind is democratisation - not necessarily global networks of interventionists doing procedures across the globe. I don’t think they mean that Alaska will beg operated on from Alice springs. I think they mean remote areas will be connected via local regional hubs. (Just my take.)
Our First In Human Procedures
In November and December 2024, Remedy Robotics achieved a significant milestone as we performed our first cases in a human with Dr. Vitor Mendes Pereira and his wonderful team at Unity Health in Toronto.”
Right Nov 2024 to Dec 2025 is a lifetime in health robotics - and this is their latest brag on procedures which maybe tells me there is a little rethinking going on… more here.
“The procedures were entirely robotic, from catheter placement into the femoral sheath through withdrawal of the catheter back into the sheath. The way it should be.”
Okay this is a highlight I really want to bring in here for a few reasons. So firstly there are two schools of thought coming - one is - “it’s about the navigation and getting where you need to go and let the robot and AI help you get there.”
The second (remedy is in this school and they are not alone) is to do the whole thing soup to nuts (for this not familiar A-Z). So from placement to withdrawals should be done using the robvoic system. Look at this image.

It has a massive area blurred out - which means to me big robot. Why do I think a big robot (see Sentante vs Corindus later) because if it needs to do insertion - removal exchanges and driving all of the catheters and devices - not just the guidewires - it is a very different form factor of robot. Plus if this is to be done “over the wire” it changes the form factor of the robot.
And let me just remind those less familiar; that if you did cardiac with rapid exchange guidewire manipulation that is a very different challenge to being able to do over the wire exchange. And I’m suspecting that this may well handle OTW judging by how much is obscured. BUT I have been wrong before.
(I will, during 2026, do every company in excruciating details - patent trawls - and I’ll be visiting a few of these companies by kind invitation.)
They continue: “These first in human cases represent a critical step in our clinical trial program that will prepare our system for wide spread deployment as we pursue our goal of bringing flawless and immediate endovascular care to every patient, no matter where they are in the world.
Surgical robots are only worthwhile if they leverage best-in-class technology and deliver transformative improvements inpatient outcomes, and we are incredibly proud to see our technology start to make a real difference to patients. This is just the start.”
So “Flawless” features multiple times and really starts to lean into the AI and ML side of this. Like many of these companies - that assistive navigation is what may make the difference here. Not just in NV procedures - but it can also start to help in complex CV (Coronary, valve, ablation robots) and in the wealth of complex and tortuous PV (peripheral vascular) procedures.
Robocath / R1 Microport
Got a little slap as on my 9 box of robotic companies I didn’t have RoboCath. But be assured they have always been on my list. Especially as I was out at Microport - Medbot earlier this year and it was a topic of conversation.
Some background: Robocath is a French vascular-robotics company best known for R-ONE, its robotic PCI platform designed to give interventional cardiologists precise, radiation-free control of guidewires and balloons during coronary procedures. The system matured steadily in Europe, but Robocath’s real expansion came when it partnered with MicroPort’s robotics division, MedBot, to create a joint venture in China. That JV, often referred to as CathBot, combines Robocath’s technology with MicroPort’s regulatory, manufacturing and distribution muscle inside the world’s largest PCI market - China.
Through this partnership, R-ONE secured approval in China and is being used in clinical practice, supported by locally run multi-centre trials and a push toward broader commercial rollout. The relationship is symbiotic: Robocath gains access to a scale it could never reach alone, while MicroPort gains a mature vascular-robotic platform to plug into its growing surgical-robotics portfolio. Together they’re also developing next-generation versions aimed at remote, 5G-enabled procedures and broader vascular indications. (Broader indications folks.)
In short, Robocath remains the technology brain, MedBot is the commercial engine, and China is now the centre of gravity for the company’s growth, as far as I can see.
Right so one might be forgiven for thinking this is a pure cardiac robot. BUT like many systems - and I want to keep reinforcing - once you are in the vasculature - you potentially can go anywhere - and they have headed towards the brain with carotid artery stenting. (CARE study.)
Now purists will say “Piffle” if they come from 19th century England. That’s not Neuro. Well it’s not Intracranial but it is neuro to many. But what it shows is the pivot - as honestly - I am not 100% convinced of a pure PCI robot anymore - but am convinced of applications across PV, CV and NV.
(Do I keep saying this?)
The PV - CV - will be bread and butter - everyday procedures - the NV will be as this blog has been about. And I am more convinced that being able to do all procedures will eventually be the unlock to having a remote regional telerobotic neurovascular set up at scale. As it will really make the economics and the “proficiency” more attractive. BUT I COULD BE WRONG !!!!!
One question will be - “Is it better to start PC / CV and head to the brain as a company? As you get to test your system in less frantic circumstances and potentially (sorry) easier procedures?”The other view is - “If you can do the complexity and speed of NV in stroke and Aneurism - PV and CV is a walk in the park.”
I can literately hear air being sucked between teeth.
Sentante
I’ve met the CEO Edvardas on a few occasions at meeting like LSI. The team and idea originates in Lithuania and I heard about it when it was in its infancy. Since then a lot has happened.
But let me first dig into why I was intrigued by the device.
As you can see it looks very different to any of the roller based mechanisms. Sorry I didn’t want to get too technical - but

You have all kinds of ways you can manipulate guide wired and catheters. You can use standard guidewires and catheters and have rollers that Push N Pull and twist (torque) the product.
You can have proprietary catheters that are hydraulic or cable driven with push and pull mechanisms.
And you can have grasper based (for a better word) push n pull and rotation that mimics the human hand and finger grip. Which is where Sentante have gone (Sorry Edvardas I probably butchered that after your great explanation the other day.)
A picture speaks a thousand words.

So let’s say there is the bedside control system and then there is the user (console) control system for most types of system. And out there today are joysticks - mouse like track balls - dials and… interestingly for Sentante a “wire” controller that simulates normal wire control for the use. And more so it is a haptic (1:1) controller.
Why have they gone down this route? - Because they want to mimic how it works and feels just like would happen in the Cath lab. Push and pull is the same - rotation / torque is the same. And they said to me they have a direct 1:1 realtime feedback of the haptics. Local lag is almost zero on the system - and transatlantic lag is sub 120ms - which by all accounts should be imperceptible by a user.
One of the worries with some of the mechanisms (real or not is till to be decided) is that you can push a joystick hard and get into “fast” modes on some systems and that can overshoot junctions or even perforate vessels. Sentante is thinking - replicate what they do today - and give haptic feedback. Works and feels just like they know today.
BUT if you have the mass of sensors they claim in the system; and collect all the kinematic and system data - you can start to give user feedback - and train AI - and get “co-pilots” to avoid those dissections and perforations and improve accuracy and speed. They believe you start with how you do it today and then add co-pilot assistance to help users. I think this could be important in younger trainees to give them graded assistance.Add into that they believe strongly (we talked a lot on this) that NV is the grail but the PV and CV makes it a economic workhorse for the rural spoke hospital. And that seemed amplified by the fact that say (within some ranges) any guidewire - any catheter - and device (and up to 4 controlled at once) including all the fluid management - all from your shielded seat.
For sure it has me intrigued - and for those interested - they are raising money now to launch in 2026 in Europe for Peripheral Vascular - and to move toward NV.
Lots going on.
Shanghai Aopeng Medical Technology – ALLVAS
I’m not going to cover every single Chinese endovascular robot. There are many - many in development.
Others names out there:
Denuo Brain Neuromedical Technology (Hangzhou)
Genlight Medttech (Hangzhou)
Rainmed Medical (Suzhou)
Vas Medical (Beijing) / Wansi Medical - VAS Robot
I just picked this one from a list as it had the most info I could scrape:
Aopeng Medical, based in Shanghai, has built ALLVAS as a universal endovascular-intervention robotic platform aimed at coronary, peripheral, neurovascular, and aortic procedures. (Another one that sees value in being broad.)

“ALLVAS distinguishes itself by being compatible with standard off-the-shelf catheters/guidewires and stent-delivery systems rather than requiring proprietary disposables — a “platform-agnostic” design.“
So we see here again this schism between - proprietary and “off the shelf” devices like guide wires and catheters. I think this is going to become one of the interesting sides of this technology as it plays out. Does using any catheters keep it too generalist? Or does this strategy allow the latest and greatest advances (by any catheter company) to be “just used.”
Does it allow freedom for hospitals in contracting?
Or, on the flip side, does proprietary mean “it works better because it’s custom.” It is tuned for the robot, All yet to be seen. Let’s not forget Intuitive have build a multi billion dollar company based on their own proprietary razor blades.
The challenge that companies using any other companies’ consumables is that you are potentially leaving most of the profit on the table. And that financing and financing models may become a competitive deciding factor.
If I get the system for free- just by using “your disposables,” that don’t cost a lot more - is that choice of devices something I’m willing to give up? Especially if it works so well with the robot.
Or am I so ingrained and invested in my products and relationships - I am not changing for anyone. Instead I’m willing to pay the hardware - and to hell with the forced switch over?It will be a critical battle as we are not talking here about “accounts” switching over we are potentially talking about entire networks. And trying to get every user in every part of the network to switch over should not be underestimated.
Back to the robot: The system uses dual multi-manipulator arms to control catheters, guidewires, and even stent-graft deployment - enabling full procedures like EVAR (endovascular aortic repair), peripheral vascular interventions, and potentially neurovascular interventions.
And like most - under remote robotic control from a protected console. And I would presume long distance - because China is the absolute leader in this today and has some of the biggest needs for remote surgery of all types.

In 2021, Aopeng reported first-in-human use in iliac artery intervention, and shortly thereafter completed thoracic and abdominal aortic aneurysm repairs with ALLVAS, marking it as among the first robotic systems worldwide to perform complex endovascular graft deployment in humans.
More recently (2025), a lower-limb peripheral arterial disease (PAD) series documented successful robotic-assisted interventions without manual conversion, with good safety and dramatic (> 95%) reduction in operator radiation exposure. ALLVAS remains pre-commercial on many fronts, but it represents one of the broadest, most flexible, and most mature non-US endovascular robotics platforms - with (according to them) a design philosophy that prioritises device compatibility, full-procedure capability, and workflow practicality.
And they are not alone…
Siemens Healthineers & Stryker
Okay - let’s move to the big elephant in the room, and the news that broke a few weeks ago.
This - in part - is why I chose to drop this blog now, and why I see now as the time for right time for neurovascular robotics.

Siemens acquired Corindus for cardiovascular applications a few years ago. But to be honest - from the outside - have had disappointing results. Some say it’s not a great design etc etc. But I look at it like this:
Not enough patient benefit to be a must have. The protecting of the users from X-rays is good for the user but not for the buyers that never go near an X-ray source. Complexity and cost didn’t justify the system. In effect a hard sell. Note: I think that is changing - the avoidance of radiation and protection of staff is rapidly climbing up the management table of concerns.
Plus at that time data - AI and telesurgery were still nascent ideas. Far off dreams.
Roll forwards to today and Corindus (shame about the name if they keep it: Cor - coronary) has decided to head to the brain. As I think Siemens Healthineers have understood that is where a real patient difference can be made. And to be honest they have done it in a smart way.
You see if you are a company of “big Iron” you won’t necessarily have the know how, competency and teams to build the devices that are needed if you want to have a razor blade model. So step in a leader in Neurovascular - Stryker.
Stryker not only own the devices and procedures in Neuro - they also own the environments where they are done. And I start to see a very interesting (but not friction free) pairing up here.
Between Siemens and Stryker they could literally dominate the entire Interventional Neuro suite - between imaging and peripheral devices, connected systems, lighting and infrastructure. They both have the muscle to do this. In combination it could be quite formidable.
Now it could cause the “You have to buy Stryker devices” that may irk some people… but this feels like the route they are going down. And for the businesses it could open some interesting contracting - building of infrastructure and networks, as well as unlock some profitable business.
With each company bringing a serious know how in each part of the equation.
Is the current Corindus device suitable for NeuroVascular?. Hmm.
It’s a rapid exchange system - and has some technical characteristics I will cover in posts next year - that means it pretty much (in my mind) needs a total redesign.
But they have done some neuro cases historically with the system - but I’m not sure its as optimised as it needs to be.
For Stryker it’s Gold, and it comes from wisdom. “Corindus” is not their Stryker’s venture into robotics. And I’m sure their experience with Mako has led them to “Let big iron do the iron and imaging and all that.” Stryker will focus on the surrounding products and services - which they do so well; without having to invent from the ground ups. robot.
So for me, why is this potentially one of the most important news items of the past year for this sector? Because out of this whole list - they are the first major strategic (strategics) to validate the space.
They have basically said “Endovascular robotics and neurovascular is thing. A big thing.”
This could trigger other big players (as I intimated about before) to move on this space. And the list is distinguished with some players like JNJ, Medtronic, Microport (already in but focused on Toumai), Penumbra, MicroVention (Terumo), and a host of other Neuro companies to look at this space - maybe partner with the robots in this list.
My bottom line is (as always) the smaller companies can move faster - but it will be the big companies that survive the marathon to the end of the race. And they will ultimately set the direction of the industry and buy up the best of the best.
Stereotaxis
Lower on the list - but that is just because of alphabetic. As when most people think of navigation by magnetic catheters they immediately talk about Stereotaxis.
Stereotaxis is the long-standing pioneer of magnetic navigation for endovascular and cardiac procedures, best known for its big-iron Genesis and Niobe systems that steer magnet-tipped catheters using external magnetic fields rather than mechanical push–pull.

Stereotaxis feels familiar to everyone - well the name - because they have been around for almost 35 years. And that is good and bad for the industry here. Good because they’ve been around a long time so magnetic navigation is not new - bad because they can make people think that whole area of magnetic navigated guidewaires and catheters is actually stale.
As an investor - through the stereotaxis lens you could say “Been there done that … move on.”
But I am a firm believer that 50% of any technology is timing. Da Vinci was honestly a curiosity of just Urology for a long time. But the real explosion in robotic surgery has been since 2018 - where it suddenly became, the main stream. General surgery and gynaecology got technological advanced (X Boom, Stapler, Advanced energy, ICG) that really made it a must have.
I think Sterotaxis was just “too early” but now… it’s potentially different.
Historically rooted in electrophysiology, Stereotaxis has been positioning its platform as a general intravascular navigation technology, with recent work extending into vascular and even early neurovascular research models. So they are yet another that potentially sees the need for multi specialty in endovascular.
The pitch is the same today as it was at the start: ultra-precise, fatigue-free, radiation-safe catheter navigation from a remote cockpit, with the promise of more consistent outcomes than manual techniques.
Commercially, they’re still primarily an EP company, but their technology remains one of the most mature non-mechanical navigation systems on the market - and is often cited as a potential springboard for next-generation remote or AI-assisted vascular navigation.
Still one to watch.
XCath
Last on the list (It was just alphabetic Eduardo!) - I’ve had many conversations with CEO Eduardo Fonseca. Who also happenes to be CEO of Endoquest. Hmmm.
XCath spun out of the University of Texas Micro-surgical lab, which was founded in 2014. It spun out as a private company alongside EndoQuest Robotics in 2017. They both have campuses in Houston and South Korea.

They sit in the “serious contender” category of next-generation neurovascular robotics, because it isn’t trying to reinvent the stroke workflow from scratch - it’s trying to make the hardest part of it controllable, repeatable, and remote.
The company is built around its EVR (EndoVascular Robotic) system, which uses a highly precise mechanical drive to control ultra-flexible guidewires and microcatheters deep inside the cerebral circulation.
Unlike autonomy-first concepts, XCath focuses on giving the operator extremely fine, stable, fatigue-free control of distal navigation in tortuous intracranial vessels, while staying compatible with the devices clinicians already use. This practicality is a big part of why they’ve jumped ahead of many early-stage players.
Again - another company that is using - “Off the shelf” to limit friction. And to possibly make the system deployable anywhere.
What may have just changed the game for XCath is its first-in-human milestone: in Nov 2025 the team completed robotic-assisted aneurysm procedures on real patients in Panama using their EVR system. These weren’t phantom trials or animal studies - these were true intracranial aneurysm embolisations, with the robot navigating microcatheters to the aneurysm, deploying coils, and completing the case without manual conversion. Of note was they were completed robotically without the need for proprietary consumables. All off the shelf. (Note: They can handle 3 devices at once - so can control the whole procedure from the console.)
Again - it is this “open architecture” that keeps coming up. And I’m starting to think it is important. Perhaps to get true scale for these robots - the clinicians need to reach for what is on the shelf.
What makes this even more notable is that the team carried out the procedures using a monoplane angiographic system, rather than the biplane setups most neurovascular operators rely on for spatial accuracy. This is big - and important for being able to do this in any lab. No specialist equipment. No need to buy a biplane imaging system.
The fact that EVR could deliver microcatheters and devices into the intracranial vasculature under monoplane imaging speaks to how stable and controlled the system’s navigation must be.
These cases have put XCath into a very small club of companies with live, real-world neurovascular robotic procedures, and arguably positioned them as the earliest mechanical neurovascular robot with actual human data on aneurisms.
The platform is also being framed as remote-capable. XCath has signalled plans for tele-operated stroke intervention, where expert neurointerventionalists could robotically perform aneurysm or thrombectomy procedures from a distance. Which is the entire hub and spoke model I have discussed above.
Their pitch is that the EVR system offers sub-millimetre navigation stability and smoothness far beyond manual hand control, reducing operator variability and enabling safer access to distal branches - something interventionalists struggle with even after years of training.
Why? Because in part the coatings on Gudiewires (go see the video on guide wires above) make it more difficult to get slip vs control. So it’s important to know that XCath developed a 0.014 steerable guidewire using electro-active polymers. It is this guidewire magic that they think makes the difference.

Early data from their preclinical and procedural work has shown consistent success rates in navigating highly complex anatomy. The reason that problem is so hard to solve is that the hydrophilic coating of different devices reacts to vessel tortuosity in unpredictable ways. The solution may rely on material sciences and not on just robotics.
Where they are now is early but potentially meaningful: XCath has proved feasibility in humans, is working on expanding procedural indications, and is preparing for broader trials to support regulatory pathways. They’re still a young company, not a commercial player yet, but they have what most neurovascular robotics startups lack to date - proper in-human intracranial cases. And they did back to back cases in the same day.
And let’s not forget that aneurism may be the hardest part of any of this with the smallest vessels and most complex procedures. They probably think that if you can crack the aneurism procedure - everything else like Stroke is a magnitude easier. Let’s see.IOt is clear they believe you go head first and head for CV and PV later when you’ve cracked the hard nut.
XCath is already positioning EVR as “the only neurovascular robot currently in development that has achieved full intracranial navigation and treatment in humans.”
They have shifted from “promising concept” to “demonstrated clinical reality.” If the next wave of cases continues to show safety and consistency, EVR could move rapidly from early clinical feasibility toward being a serious contender for the first broadly adopted neurovascular robotic platform.
That alone makes them one of the most important companies to watch in the space. And as they might be raising money soon… Investors might want to reach out to Eduardo.
others in stealth mode - UN&UP (corBot & Thrombot), Route 92 medical
Summary on Endovascular / Neurovascular Robotics
I don’t know about you but I’m tired by all that. This has been one of my biggest (and I feel most important blogs.) Important for industry but most of all important for what we might see with patient care. Please share this blog wide if you got value from it.
Why have I spent all this effort here today? Simple - first and foremost I think Stroke and Aneurism is so important. To put it in perspective are the patent numbers - Stroke is one of the biggest medical burdens on the planet: more than 12 million people suffer a new stroke every year worldwide, and over 300,000 of those are ischemic strokes in the United States alone. Of those, only a small fraction ever receive mechanical thrombectomy; even though it’s one of the most effective lifesaving procedures in modern medicine.
In other words, tens of thousands of Americans who could walk out of hospital after a stroke simply never get access to the treatment in time. And that is replicated across the world.
Aneurysms tell a similar story. Around one in fifty people has a brain aneurysm, and roughly 30,000 Americans a year experience a rupture. Half of those patients die, and of the survivors, two-thirds are left with serious long-term disability. These aren’t rare conditions, they’re high-volume, high-impact emergencies that still depend heavily on geography, specialist availability, and the sheer luck of whether an expert is standing in the right room at the right moment.
I can’t say it any more bluntly: neurovascular disease isn’t niche. It’s a global, high-frequency, high-mortality crisis; and it’s exactly the kind of field where expanding access, increasing capacity, and bringing consistency through robotics could change outcomes at scale.
Let that sink in!
Now from an industry side - and investors - you might want to listen up if this is all new to you!I believe, neurovascular intervention is sitting exactly where laparoscopic surgery was before Intuitive Surgical exploded: a high-volume clinical need bottlenecked by specialist scarcity, uneven access, and workflow complexity.
Stroke alone generates hundreds of thousands of eligible cases in the US and millions globally, with reimbursement levels that dwarf most soft-tissue procedures. Yet unlike abdominal robotics - where Intuitive grew into a $120-billion giant by capturing elective surgeries - neurovascular care is an emergency market where every minute is reimbursable, defensible, and economically justified.
The gap between the number of patients who could receive thrombectomy and those who actually do represents billions in unrealised revenue annually. Add aneurysms, AVMs, tumour embolisation and peripheral neurovascular procedures, and you get a total addressable market that rivals early Intuitive-era general surgery - but with far stronger clinical urgency and far less competition. The first robotic platform to reliably extend expert-level stroke and aneurysm care to hospitals that currently can’t offer it doesn’t just save lives; it unlocks one of the last unscaled frontiers in interventional medicine. This is what an “Intuitive-before-Intuitive” moment looks like.
These are simply author opinions scraped together from various sources. It’s scope is education and solely education. It can have errors - I’m human. So if you spot something that’s a mistake - let me know - I’ll correct it

