
The Arms race in surgical robotics - why they are so important in design choice
- Steve Bell

- May 28, 2025
- 22 min read
Updated: Aug 6, 2025

Back in 2014 when asked to go visit Cambridge Medical Robotics (the original name for CMR Surgical) I was hesitant. Very hesitant. All of my being said to just leave Intuitive to that game: as no one else could really win against them.
Over a period of weeks I was convinced to come and see CMR and the prototype they had been working on.
When I stepped into the lab up on a hill above Cambridge (gorgeous location by the way) I instantly understood that arm architecture can change everything.
In the last decade of my journey with surgical robotics, I’ve understood so much about what critical components make all the difference. Instrument and instrument design. Controllers, cockpits and the interfaces that the surgeon uses.
Imaging systems, energy systems and ecosystems.
And everything is important of course - from the tip of the instrument that interacts with the tissue to the plug that goes into the wall to power the system. It’s all important (to a degree.)
But it’s the arms… the arms that for me are one of the three key things on a robot that matter and determine the very experience - shape - deign - ethos and philosophy about a robot. The most important.
Today we see a varied pantheon of arms. From the classic Intuitive mechanical remote centre and Z-rail design, to the V-wrist of CMR, to the suspended swivel of a RobSurgical, the micro arms of Virtual Incision, the elbowed flexible arms of the SP, and the bed mounted arms of Ottava.
The design of those arms - and how they get the instrument to where it needs to go. The design in the load delivery of the arm - does it hang from a boom or does it sit on a cart, are they attached to a table, or even do the arms sit inside the patient.
That one design ethos changes every single aspect of the robot. And in robotic laparoscopy style operations - often with multiple arms - it really matters.
I’m not an engineer - but what I want to do here is translate some of that engineering into what then happens in the real world. And why engineers should be paying attention and thinking out of the box.
So why is the arm so important?
On the face of it this may seem like the most stupid of questions - right? (I’m known for them.)
But day after day, I see designs appear that simply mimic the da Vinci arm in one form or another. As the mechanical remote centre must be the winner “right?” I mean it has successfully done 16 million surgeries. So it must be the right way to go.
Well yes and no. Because with that form factor comes very big compromises I will get into later. But also if you just clone and Xi - that will alienate many - and many will say “give mew the real deal.” It doesn’t automatically set you up to be different. Which through personal bitter experience can be both good and bad.
In the simplest form - the arm design and how it moves will determine how the instrument inside the patient will move. Let’s take the most common types of arm. These are the classic da Vinci Xi style arms. And for this exercise we have to start at the end with the instrument and work backwards.
The instrument (in most robots) is woking through a trocar - well technically it’s not, it’s working through the cannula of the trocar - just to be picky. And that cannula has a pivot point within the abdominal or thoracic wall.
So in effect, the instrument is just a lever through a fulcrum.
If the instrument is deep inside the patient, the longest part of the lever is past the fulcrum (or pivot point) so that moves a lot inside the patient for little movement outside the patient.
But as the tip of the instrument moves back towards the pivot point (or Fulcrum) more of the lever sticks out of the patient; so small movements inside the patient = big movements outside the patient.
Now point 2… and this is important. The da Vinci style arms hold the instrument on a rail. The Z- rail: and the instrument slides up and down that rail. That’s how it goes in and out inside the patient (the Z axis.)

So if you now fix the depth of the instrument in the patient (the Z axis is fixed) and you want the tip of the instrument away from you (moving the X or Y axis) - via the lever - the whole Z rail comes closer towards the boom of the robot. But if you want the tip of the instrument near to you - the Z rail has to move away from from the robot. And if you want to replicate that when the instrument tip is up near the abdominal wall - it needs to move a long way from you. The lever effect.

So depending on how big you want your effective working space (like inside the abdomen and how much of that you want to be able to reach) you can end up with a big volume of movement needed for the tip of the instrument. From deep on the pelvis at the dentate line to say up at the oesophageal junction and the crura muscles. Plus lateral to lateral boundaries.

** I’m going to hop up on my soap box for a minute here - and hopefully give some deep guidance to companies and teams.
In the past 10 years I’ve seen a deep degradation in the anatomical, surgical knowledge of teams. I expect during this article that if I discuss anatomical landmarks - anyone reading this or in their team must know where they are. (Not talking to clinicians here) - but company folks. If you don’t know the anatomy, physiology, or surgery of the field you are in… you need to get knowledge hungry NOW. **
So, from top to bottom - side to side - deep to superficial - that instrument tip can move through a vast working volume. And if you want to do that with a da Vinci arm… then that Z rail needs to be quite big and long to allow that instrument tip to move through the whole volume. And the bigger and longer and then “heavier” that Z rail is… the arm structure that delivers that payload needs to be longer - stronger - bigger and heavier. So the part of the arm that delivers that longer stronger part of the arm needs to be longer - stronger bigger and beefier. And the Structure that holds that arm (be it a boom or a cart) has to be bigger and heavier (to not tip over) and have a bigger wheelbase for stability. It’s how you end up with big trapezoidal arm structures.
And that’s why any current technology that uses that type of Z rail arm is normally quite big and heavy. It’s just the nature of holding the instrument like a dagger. And if you simulate that at home - grab a long stick - hold it like a dagger and then hold that stick with a pivot point and try and move it like a lap instrument. You quickly run out of arm reach.
So HTF do surgeons manage to do that in laparoscopy? (You should be asking but with less swearing…)
Simple peeps… look at how they hold an instrument. They don’t hold lap instruments like a dagger (or a da Vinci.) They hold it like a sword fencer. And if you watch a sword fencer - they can make the tip of the sword get where they want it to with just the “Flick of the wrist” - wrist. Wrist.
NO not the instrument endo wrist - but the wrist of their arm.
Grab your stick again and now hold it like a conductor, or a sword fighter, or Harry Potter fans like a wand (Laporiamus). Now move that tip through the entire working space of the abdomen - and low and behold you never run out of arm length. Like most lap surgeons.
(NOTE WELL modular users - you may well have to move your body a bit to be in a comfy position. Cough cough - no single docking of modular arms… cough cough.)
But your wrist as a human means you have a very very very different movement than the Z-rail of a da Vinci style Xi.
That is where there was genius by Luke Hares at CMR Surgical. He completely understood that… and “in thinking to mimic the way lap surgeons work” he realised that a 4 axis (V-Wrist) was needed. A very very different arm to that of the da Vinci. Your wrist allows your hand to pitch up and down and yaw left and right.
And that is why the arms of a Versius as so very compact - yet it can do laparoscopy and Thoracoscopy so well. And the arms are slim - and the system is smaller and lighter than other modular robots. Yet never tips over - and can reach everywhere (even with shorter instruments in total length) - but that’s a more nuanced talk maybe for another day.

In short (pun intended) Versius has a different arm design… and that changes everything about the way it works. It is also co-botic (you can push the arms around it’s very friendly to be against) and and and - ta da — that wrist design and elimination of the Z-rail means you can put the rotation of the “hand” the part that holds the instrument - in that hand. So the choice of arm design changes so much.
But so what?
It’s a lot about rotation
It’s missed on a lot of people but the rotation of da Vinci like wristed instruments is a marvel of engineering. However, it requires some very clever mechanics inside. You see down each instrument run sets of cables for moving the endowrist - pitch / yaw / grasp. Plus some flushing tubes; and in electrosurgery instruments - the power wires.
That uses three small wheels at the back to move those cables and get the tip of the instrument to what you need it to do. No mean feat - and I will do a full deep dive on this for all the instruments types out there, and include non cable instruments etc etc another day. (So keep the subscription!! My kids need shoes.)
But the there is also another little drive wheel that turns the entire shaft of the instrument relative to the housing that clicks to the robot.
So this total combination gives you pitch - yaw - roll - with the Z rail controlling how deep the instrument goes into the patient.
But adding roll in the instrument means only slightly more complexity at the robot end - more drives and more interfaces. But what it also means is that when you roll the shaft of the instrument all that lovely cabling down the shaft gets twisted as it rolls.
And like watching a swan swim you don’t see the little feet kicking under the water. The control algorithms needed to take into consideration the changes in cable tension so that as you roll you don’t get odd unintended movements at the endowrist is phenomenal. And don’t get me started on force feed ack while rolling……
And at a certain roll limit you can’t twist any more. You reach a roll limit - 500 degrees to 760 degrees depending on the systems. Ever wondered why they have a roll limit. Well for the Z rails… now ya know.

But all that fancy footwork in the instruments is a direct result of the design of the arm and the use of a Z - Rail. And interestingly most industrial robots don’t use Z-rails for that reason, as they need infinite roll. But then again they don’t usually have a lot of arms so close and they don’t often have people standing between them so a Z rail os seldom needed. I digress into co-botics for a bit later.
Where as in a system like Versius - all that roll complexity is in the robot arm (because it ain’t a Z-rail folks) so Versius instruments don’t need roll and all that complexity in the actual instruments. That’s why they are smaller - that’s why they are less complex. The roll is in the robot.
But you keep all the pitch - yaw - grasp - and roll. Just in a different way. Due to different arm design.
RobSurgical and Asensus (Senhance and Luna) have done similar things. The roll is in the terminal joint of the robot… not the instrument. And they both have approached getting a robot sort of wrist on the arm in very different ways. Take a peep here.


Okay you want to know about Ottava - everyone wants to know about Ottava
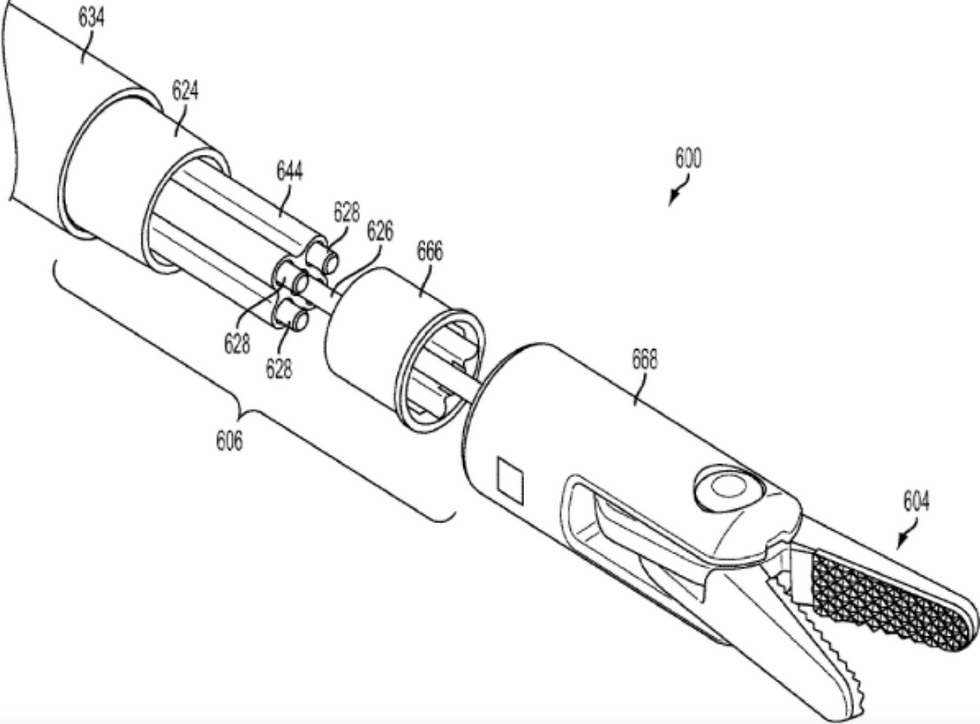
Well there’s a very interesting one, and I know nothing you don’t know. But I spend time to read patents and look at images in more details than a normal person should. You see Auris had an original design much like Monarch where the instrument ran through the centre of a cylinder end joint.
I saw the patents and I saw the released images that were on twitter a long while back.
Clever… as you get rotation from the terminal joint of the arm by spinning the whole instrument - And what was more interesting (see images) was that the Z (in and out) was controlled by that end cylinder. So in effect you took rotation our of the instruments - and removed the Z motion from the robot arm all in end joint of the robot.

A super smart idea and technological marvel in how you controlled cables in those types of design (tensioning) - rotation etc etc. But all of that means the end joint gets bigger and wider - the more you try to do everything in one unit. A unit that is in there operative field.
So understand that the end joint actually connected to the top of the cannula of the port, and became like a sit on “valve control cap” of the port. And the beauty of that design was that you basically only had the movement of that end joint to get X & Y movement of the instrument. Tiny - small delicate movements. In theory.
Plus the Z rail eliminated and the instrument doing all the Z movements meant that the arms that delivered that end joint were slim and light and would hardly need to move.
They did the opposite of Z rails and brought everything as close to the patient as possible.
Alas - everything has pros and cons. On the day I saw the twitter picture I proclaimed - FAIL !
Why?
Because to me it looked like you could never get the trocars close enough for real life surgery. The final joints would almost always clash in many set ups. So port spacing would be need to be very big. The end joint diameter would set the lower limit of spacing. Next seems that to get real surgery angles (especially now the ports need to be placed at large spacing) would in small patients - or very obese patients - or thoracic - possibly dig into the patient to get the angles. It would put some limits on the movement - well in my mind.
But to be honest I think it was the ambition to do it all in one joint that killed that design. You see that form of round end joint with a hole through the middle was the Monarch style and hence you could get flexible robots through - just it like Monarch - so the six arm design would have allowed the rendezvous procedures I touted in various posts. Super cool and super ambitious and everything works in powerpoint.
But again - to anyone that has lived and breathed this - sees the reality of boiling oceans in this space… And the reality of in OR use. And more so - the complexity in that end joint must have been off the charts (smart and cool engineering) but not a product you could probably make at acceptable costs (my diagnosis) to make a profitable business.
And those self tensioning interfaces - extra cables - mechanisms - very very cool - but instruments being able to be made en-mass… for realistic costs? How much would that cool design cost in reality and could the market support it. Or could internal margins accept it?
My diagnosis (and I’m speculating here) is that Auris design could win in a one off lab - against the Verb design. BUT the reality of production, costs, real world use would have been the killer of it, at a guess.
But that Auris design would have meant that bed mounted would have had smaller slimmer payload arms because it didn’t need to carry a big Z rail. I think reach could have been quite impressive as you don’t need to “reach over - ever. Or even move a lot during surgery. So the Kinova arms I saw in early images on Twitter would have been super nice (but the rail mounted at the side of the bed was goofy. No offence.)
But what that design shows is another good approach to eliminating the Z rail - associated travel needed and the need for big payload arms. It was smart and a shame it couldn’t be realised.
My fear on the Verb system (and only from what I’ve seen in patents etc) is that they went for the original design of Z rails mounted on bed mounted arms. And even if a bit smaller than most Z rails (perhaps?) - the payload arms that will come from under the bed to come up and over will have to probably be a little bigger than the original Kinova arms… and may need to move a bit more and and and. I am hoping that the addition of Z rails - and reality of clinical use will not require even bigger payload arms.

We wait and see as early cases have been done and I’m hoping to hear good news soon. Images are scant - Like below but those arms look quite big. But huge should out to the engineers for getting all of that and the end joints under a table.
The other issue I’ve always wondered about that Ottava design has been that you end up needing in 8 DOF (degrees of freedom) from my calculations. And you basically end up with almost 2 robots in each arm. (I can be wrong on this). But a payload delivery arm that gets you from under the bed and then up and into position with enough reach. And then the “robot” business end with a Z rail - which will mount to those arms. I might be hallucinating though so don’t hold me - but the Verb patents point to this kind of “double” robot arm. That is complex and expensive to make.

And if that is the case… I do start to wonder about any realistic Cost of Goods on such bespoke arms. They could be really really interesting. But Table - complex arms - gorgeous looking console - high end modular tower (my big speculation from this post — https://www.howtostartupinmedtech.com/post/dualto-is-a-sneak-peek-inside-ottava)….. very high end instruments from JNJ for sure.
I cannot see any way that end pricing of that beauty can be less then $2 Million. And if that is the case - it’s a potential challenge to make a viable business work. Pricing is falling rapidly per case and — capital is being placed in deals. Placing a few hundred high end systems starts to become prohibitive even for a JNJ. Unit cost economics do not favour placements when starting up.

But what I love is that they really are thinking out of the box on the arms. This is a hybrid design. And I imagine it will be co-botic. I mean if it is at the bed - it has to be.
Robotic or co-botic
I’m not an engineer so why are you asking me? But I am someone that has been “touched” or “whacked” by most systems at one time or another.
You see one of the issues of Z-rails and the large external arm movements is that when the tip of the instrument is up near the abdominal wall - if you want to move that tip from side to side (due to the lever effect) the outside arm needs to move quite fast. And if something gets in the way - like another robot arm or a head… you can have a serious clash event.
The more mass you have up on the instrument drive pack, the longer the lever, the more momentum you get. The more momentum the more risk of overshooting, but more so doing damage.
In fact all the arms are designed with safety limits on speed and motion and collision. This reduces the risk of serious injury. But having been whacked by arms - it hurts and I would not want a full speed one to the head.
And if they clash (bigger and longer the arms… more chance of clash) + (more movement needed more chance of clash) - then that can create a safety event where the system faults. And annoys the surgeons a lot. And if it is a big enough smash - it can trigger a red alarm where the arm needs to be checked by an engineer that is hasn’t been damaged. That is a potential case stopper.
Or even worse if it hits a bedside assistant…the bedside assistant removed and replaced if ya get ma drift.
Of course there are sensors and crush strips and all kinds of things on the robotic arms… but more recently there has been a move to co-botics.
I’m gonna get this wrong; I know some bright engineer should correct me. In a car factory big robot arms are swinging around at speed in defined trajectories and no one is near them. They are sometimes even in cages (Roar!!!!). And if that arm was to smash into a frail biological human - the result would be Robot 1 - Human 0.
What has been developed by many of the robot manufacturers around the world are co-bots. Collaborative robots. Robots that are very safe to be using a shared working space with a human.
They can often be pushed around by a human while they move (and they will adjust to the human). And they are often creating physical constraints and movement modes through software rather than hardware. So you can mimic different mechanical constraints through using software (sort of soft robotics in a way.)
A great example is Versius - the surgeon can be operating and the bedside user can move the entire elbow out of the way to get more space. And the surgeon would never know because the co-bot adjusts to keep the instrument tip where the surgeon wanted it. Cool - try it at a demo.

But it also means they don’t crash into someone and just keep going - they often stop - or adjust.
In fact more and more robots (in all fields) are working closely with humans so they are becoming more and more mainstream.
In 2025 if you are designing an arm (like say Moon Surgical) it has to be co-botic. It allows way faster upgrades and modes and features through software drops rather than hardware upgrades. And for many of them, it allows some very very neat tricks on how they set and adjust pivot points (Dynamic pivot points.)
Hopefully now we are seeing that arm design is so fundamental in how it works - how it delivers payloads - how it affects instruments and instrument design. How it impacts the size and shape of the robot (the robot size and shape is a function of the arm - not the other way around.)
It determines payloads, reach, and if modes can be set through software or hardware - and how things like “Pivot points” or “Fulcrum points” are set. And hence do you dock or not dock to the port.
PIVOT POINTS - RCM
RCM - remote centre of motion. A relational fixed point in space compared to the robot. Set by mechanics.
Now this has been one of the keys to the success and design of the da Vinci arms. On the trocar / port is a small black band. And this is where the port and hence instrument will pivot around. It is the pivot point or the fulcrum point of the arm; and hence the instrument that’s attached to the arm.
That point will have the smallest cone of motion for the entire system. So you want that band at the fascial layer of the patient. (If you don’t know why the fascia is important you need to.)
This black band - pivot- fulcrum point is called the RCM remote centre of motion and is a mechanical feature of the da Vinci style arm. And… of course it works. It works well.
However - when you go to Asensus, RobSurgical, CMR Surgical and others they actually don’t have a RCM. Instead they work out the pivot point at the fascia through software and sensors. The arm works out (through varying methods) where the lowest forces are at that pivot point and they set that pivot point in. Fixed point in space so that the instrument pivots through the point of least force. Sort of the tip of a naturally set cone.
Some of them will actually even continuously change that pivot point so that as insufflation changes - patient position changes - and direction you point the instrument changes - the pivot point adjust to always keep the lateral forces as minimal as possible.
Theoretically this should allow the minimal tissue damage and least amount of pain - theoretically and yet to be proven in human RCTs. But tantalising anecdotal information is leaking out that these Virtual Pivot Points and dynamic Pivot points may give less post operative pain. TBC.
So what these VPPs mean is that you no longer have to “lock” the arm to the port; which is part of the RCM. That “docking” to the port no longer exists. So I still hear docking being used and technically - well it’s not quite right. It become blurred and mixed up with “Getting the robot in position.” So even VPP systems like RobSurgical, people still talk “docking.” I think we need to upgrade much of our verbiage around robots. I’m on it… because it matters. Especially when we start to see even more wild robotic systems coming.
Put the arms inside and more…
There are some pretty radical arm designs and thoughts —- how about Virtual Incision where they got rid of the external arms - and just have a “shaft” that sits in the abdominal wall, And the arms are placed inside the patient. (See full article here)

Or the SP (single port) - where the robot arm is really now just a mass delivery system of multiple instruments through one access port. Again virtually no movement outside - unless it is moving to a new quadrant.
Eliminate the robot arms as instrument movers, keep the human in the loop and make them just pivot point holder - like Moon Surgical.
Remove arms all together, and have long flexible robots like EndoQuest (yes Endolumenal but can be technically be used through an abdominal incision.)
Lots and lots of “arm architectures or non-architectures.”
But in life there are always pros and cons to everything. Smaller or no arms and you can end up with smaller working volumes, lower numbers of instruments, less load carrying ability - less traction ability and a whole host of things I’ve discussed in many articles.
But my intrigue is how companies - and especially the next generation of arms - will develop. NO not the next batch that are currently going through IDE or MDR or emerging. I mean a decade from today. The pace of a move to affordable humanoids - will we just see two humanoids doing lap surgery? Human style arms and moving like humans but delivering lap surgery. Able to do trocar insertion and more? Never tiring and capable to set up everything and tear down everything?
What about external flexible arms. MRI compatible pneumatic arms (some in development.) I think that what we see today will persist, but we will start to see evolution - some for good usage reasons and some for “We need to be different.”
But I’m quite excited to see what’s next… what works… what can be built at the right price.
And what is going to be the right architecture as we storm towards autonomy. No longer constrained by the human replication of “laparoscopy” but next outlandish ideas that may radically change what an arm needs to be… and even should be.
It’s all about the base… ‘bout the base…
Let me step back into reality for a bit.
I want to come back to this part of the mechanism. As Meghan Trainor says “It’s all about the bass.”
Now as I discussed before - the bigger the arm needs to be (Z-rails) the bigger the drive packs (capable to drive staplers and other instruments) - the bigger the supporting arm - the longer the arm - the heavier the arm and all associated mechanics. Lead back to the base of the arms. The support mechanism.
In an Xi like device it is the X Boom. The tree the branches hang from. Needed to hold all, four arms and get them where they need to be. Plus multi quadrant. The boom needs to be big enough and heavy enough to never tip over even if all 4 arms are extended.
If you put a Z-rail on a modular system - depending how big your Z rail is and how heavy it is - will determine how big and heavy each individual cart will be - HUGO RAS vs Carina as examples.


Eliminate the Z-rail and you make the arms smaller and lighter and you get to a Versius design.
I did promise I’d talk about this so I’ll do it here. Single “dock” vs multi “dock”.
Now depending on the size of your base, and the architecture of your boom or cart - you will have a certain footprint and size. And you will have certain limits of reach.
In an Xi you put the base in one position and it stays there. One “Dock” - single “Dock.”
And surgeons get fixated on this. A single dock because moving bases from one side of the patient to the other mid procedure is a right royal pain in the ass. Cables, anaesthesia etc etc. So multiple docks becomes a very dirty word in some circles. The paradigm was with the sI you go from one side to the other side. Not really anymore with an Xi. But scars persist and for good reasons.
Hence why I want to remove the word “dock” when we don’t mean “dock.”
So if I have a modular system - and I set up the system in one configuration and then have to move the bases a little (not one side of the patient to the other side. Just enough to get optimal reach and avoid clash) during the case. (Just like an assistant would move.) some would cry out “That’s multiple docking.” Where as others might say “That’s shifting the bases a bit.”
What actually counts for the patient is time and if you need to put more ports in to do what you need to do.
The arm design - and hence base design - will all start to determine clash and position and need for adjustments. So arms are super important. And that then means that we come back to the psychology of use and “do I need to multiple dock. No way - I’ll fight on and on until I get an alarm.” Vs “We shuffle about to get best angles and avoid clash.” - big training hint here peeps.
But this critical change of thinking all stems from the arm designs. The needs for repositioning - arm design. The reach - the ports (how close) - arm designs.
And there’s more - “Can you lift the load enough” arm design - “Clash mitigation” - arm design. “Power needs” arm design. “Initial start up of the system and shut down in software” arm design. Ability to use complex instruments “Arm design”. “Arm able to hold instruments or scope and allow port hopping easier” - arm design. “Cost of the robot” Arm design. Way the kinematics work and the “feel for the surgeon” - arm design. Smoothness and the judder - arm design. Weight of the system - arm design. How it packs down - arm design. How easy to drape - arm design. It goes on and on and on.
And here’s the kicker. IF you get this wrong as the fundamental of your system - you are fucked. Simple. Because it is the critical foundation. And no amount of training, no amount of case work, no amount of marketing, no amount of cool instrument design etc etc will fix that. It all becomes a work around.
If the arms are wrong - the robot is wrong - the use feels wrong - the acceptability is wrong and ultimately the business is wrong. It will affect reliability and serviceability. Running time - faults and which parts will need to be changed. It all starts here.
In the end, who will win or lose in surgical robotics will ultimately come down to the “arms” because the instruments will be commoditised. Everyone will have endowrists that are okay. Everyone will get different advanced energies. Everyone will have a stapler (sooner than most think out of China) - everyone will have a great app. Vision systems with ICG will be ten a penny. Consoles will all become the same just open or closed with 4K screens and nice haptic controllers and smart wing mirrors.
The difference will come from the arms and the associated support base (boom or modular or table.) The surgeons feel the console and see the instrument tips and rarely think about the complexity of the arms in the middle - until the instrument doesn’t go where they want it to at the angle they need. Or they keep clashing and alarming. Or they need to put more ports in. Or they can’t have the instrument functionality they want… or or or. When an arm is working well - it’s invisible. When it’s not… the entire OR team will let you know and your robot will not be used for long.
These are just opinions and musings by the author for educational purposes


Comments