My day with HUGO RAS - but is it actually any better?
- Steve Bell

- Nov 20, 2024
- 32 min read
Updated: Jul 30, 2025

I want to start with a very important disclaimer:
My visit to go and see a HUGO case has nothing to do with Medtronic. At the AI2M - artificial intelligence meeting - I was on a panel with Prof. Matteo Rottoli - who is currently publishing a lot of good work on robotics in colorectal surgery. We got talking at the coffee break and I talked about my concerns of HUGO (well documented.) He is a big user of HUGO RAS in colorectal work.
He very kindly invited me to come and see the system in live cases at Polyclinico di Sant’Orsola in Bologna; to let me see it up close as it performs now.
The background was “It’s not as bad as you think…” And as many of you know - I’ve not been overly impressed with the HUGO RAS, so let me give some background to set my starting point for the day. And then I’ll get into a super deep dive on what I saw… and what I think.
My starting point with HUGO RAS
I come from the world of promoting modular robot arms, open consoles and differentiated systems to the Intuitive da Vinci. I am a firm believer that for many hard core laparoscopic surgeons the da Vinci style boom architecture is too restrictive vs their current laparoscopic paradigms that they find it hard (in some cases) to migrate across and integrate a “robot” into their blended practice of surgery.
I won’t go too deep here today - but it is a subtle blend of trocar positions - surgical approach, angles, awareness and a host of subtleties that mean they feel they get too dragged away from what they are very comfortable with. It is also a sensation that many hard core lap general and colorectal surgeons like a blended approach of part laparoscopy - part robotic - which creates a certain requirement for techniques and approach.
And because of that, many surgeons want an open console (so they can see the bedside and OR and robot arms.) And they want freedom of port placement - “bring the arms to the ports not set the ports to the arms.”
So as much as I bow down to the da Vinci as an incredible piece of engineering and medetch - I also believe that 50% of the surgical world would prefer a different architecture, if it’s available and works as well as a da Vinci.
Now several companies have chased this more modular approach, and open console - starting back in the day with Computer Motion. Rolling forwards to Alf-X, and CMR Surgical. And a late comer was HUGO RAS, then SSi - and next generation is Ronovo with Carina (closed console).
There is an appetite for the right modular system that allows this fluid flow between robotic and lap approaches. And allows mobility of the system between ORs (This is a totally misunderstood aspect I will not discuss today but it’s all myth.)
HUGO RAS from Medtronic, in my mind, was to be an amazing system based on DLR technology - and from the house of Medtronic - one of the most achieved medtech companies in history. I expected Ligasure, and Stapling, advanced Rubina Imaging - innovative new instruments. I was so excited as a medtech nerd - and scared as a potential competitor. Medtronic are big !!! And Powerful !!!!
I sat online at their initial launch event - and watched the system reveal in a lab. And well… I was like “What is that?!?!?”
Big - bulky with year 2000 Z rails. A clear hand held Ligasure sneaked into the video… and a photoshopped image of the system to remove a few of the wheels to make the footprint look smaller. (That’s what I thought I saw.)
It’s no lie to say I literally laughed.

Roll forward a few months and I saw it at a Congress - set up in some odd sort of “crane towards the patient way.” Medium alarms ringing across the conference centre as the system software glitched. This sent them into a “simulator only demo.” A congress with with a static robot.
I then saw a demo at an unnamed hospital where they could only get a single arm to fit into the demo room with the console.
News spread of software issues and instrument issue - some rumours and some backed up by field notices across the EU.
To me, the console looked nice - the tower massively oversized for no reason - and the arms just too big and too heavy.
I saw a live case that we eventually abandoned after software shut down after an alarm. It took an eternity to get the system back up. Docking was awkward and almost a lesson in geometry. Scissors lasted sub one hour - graspers didn’t grasp.
To say I was underwhelmed was a mis-statement. But then I saw the delay and delay for Ligasure and staplers - issues with KRINKO in Germany - and well - as everyone knows I had all but written HUGO off as a massive corporate mis step.
Now to be fair my personal contact with HUGO was a few years back - and in recent years I’ve just sort of written it off. But I know things always improve with robots.
So when Prof Rottoli stepped up and said - “Come see what we do with it…”
I was intrigued. Because the Prof and his team were doing a lot of very positive publications - and he was genuinely saying “It works.” So my scientific curiosity got the better of me to try and understand this disconnect between what I had seen - and what this team was experiencing.
So now you have the background… let me talk you though my day.
The size of the HUGO RAS system and OR Occupancy
The OR in Bologna is a decent size OR but not over sized or exceptional. When I got to the OR the system was already in place and there were four arms already draped up and pushed back from the patient.
Prof had the cart location and port set ups - up on a monitor and this was one of my first insights that I will get into way deeper later. The console was set up in the corner with the patient at about 45’ of line of clear site from the console.
I’m used to CMR Versius - so I have to say that the arm carts still seems big - but maybe I’m getting used to them - so they didn’t feel “stupid” big. But it is clear they are big. But I want to dig into this - because you can extend the arms out from the HUGO and make it look massive !!! Which I understood has been something strange in many pictures and set ups I’ve seen with HUGO. Oddly, lots of users push the carts back from the table and over extend the arms - and honestly after seeing the system better - I think that is a big mistake users might be making.
In an effort to “free up leg room” around he OR table - you end up making the system feel super massive, by having the carts further from the table. More later.
So remember, this was a major colorectal case and they had all four arms in the OR - and well - it was actually manageable, even with all that hardware.

Having a closer inspection, the build quality is excellent - and strangely it seemed less noisy than I last remember. As if they’ve somehow got the cooling fans to be quieter - but that may be an illusion.
I did note the cabling, and like every single modular system, you end up with big comms and power cables running the floor from the console / tower to the arms. No particular bad thing for HUGO - it’s an issue of all current modular systems and something I absolutely think needs reviewing. It adds an awkwardness to set up and potential trip hazards for early users. Clearly this team has worked out how to avoid the cables.
But on cables - I did note that the units were “always plugged in” from start to end of the procedure - and that does make me wonder if they can “hot swap” carts into the system - especially if it goes into alarms. Watching the way the case ended and the carts were managed makes me think - no hot swap and battery back up. Happy to be corrected.
One thing I still don’t understand is the lap tower dimensions (not the carts.). It feels super big for what it does. Almost like it was built to hold the instruments. But it had an excellent monitor - and what was nice to see was the connected Touch surgery box - and the ability to run out the video feeds to the OR main monitors and smart OR.
So I have to be honest and say that the system does occupy a lot of space pre surgery - but the tower does replace the regular lap tower - so that makes up for overall footprint.
Remember folks - the tower is power. The tower is power in 2025.
One thing I noticed was the Airseal sitting next to the tower - which I feel for this type of intervention is a must. HUGO needs an insufflator.
It's all about Docking
We’ll talk a lot about docking today - or even in this case - double docking.
If anyone goes and reads the manual for the HUGO - set up of the arms reads as bewildering. Alignments - laser markers - angles - readouts… it’s a engineer designed bedazzlement. To me the arms are just odd. But…

What I saw was the docking in - connecting the arms to the trocars - and my expectation was this this would be a 40 minute process based on the first cases I ever saw… and reading the manuals. However - this was my very first surprise (and insight) of the day.
Prof Rottoli and his team docked in multiple arms at the same time - I think at one point three were moved in together. There was a flurry off bending - moving - adjusting (and weird weird clunks) as the team expertly brought the arms in and engaged. They tested (Outside the patient) for movement above the patient. Looking for angles (translating to inside the patient) and clash. This is where my insight took real shape.
The whole procedure to dock the arms was maybe 3 minutes. But listen well - it is NOTHING like docking a da Vinci. Nothing! And that is where I’ll start to share my insights. I’m not talking the time for docking - I’m talking the positioning and philosophy for docking.
If you are a da Vinci user and you try to dock HUGO in like a da Vinci you are fucked. You will be frustrated and you will be disillusioned with Hugo.
In that three minutes I fully understood much of the criticism and push back I’d heard about HUGO.
It was watching Prof and his team position the arm joints that made me - for the first time - understand a fundamental thing about HUGO. Something I think a lot of people that use it are missing. Something that will lead to disappointment if done wrong.
Next - and this is the next massive learning I got yesterday. I noticed they’d brought the carts relatively close in to the table, avoiding the weird overreach crane effect I’d seen in the past. And there my friends is where suddenly the Hugo carts become quite compact and small.
Yes you read that right. Suddenly - when docked correctly the carts no longer occupy the entire OR. And if there is one take away for me - get your carts in closer.

The actual surface area of the footprint of the cart is not as massive as it first looks. And it has fairly useful gaps around the wheels. The lifter column is slimmer than it seems - so shoulder room around the system is actually better than you imagine. Plus with the way the carts are designed, you can step over and around all that wheel wear. And that’s ok.
If you get the carts in close - get them separated just right there is ample bedside room for two bedside assists to work the bedside. On both side of the table. And I think that was a pleasant surprise for me. Bedside real estate is not the issue for HUGO.
So fast docking in (by experts!!!!!!), close carts. And understanding how to make the arms work together with the right cones of movement outside the patient is critical. It was clear to me that if you concentrated on “internal reach and movements” of instruments. You are utterly and totally gonna mess up and get frustrated with HUGO. Because of the problems I’ll discuss next - missing this critical set up will create frustrating issues. Especially when you get to four arm cases.
Space above the patient is not great
The next part was not a surprise to me - as the actual arms of the HUGO have not changed since I saw it. They end (or start) in massively over long Z-rails - and they have a stupidly massive drive pack that swings around on it, sliding up and down. It is odd at best - a very very very poor design choice at worst. I do not like the way it moves near the bedside assist head at all.
That single design choice means that to carry that massive load - the trapezoid arms structure going from Z-Rail to cart has to be massive. So you end up with four humongous arms and drive packs filling all, the space above the patient. Swinging above the patient near heads.

A few years ago I heard Gary Guthart from Intuitive say “What counts is the airspace over the patient.,” He is so right. And to be honest for a multi arm robot that minimised air space above the patient - Versius wins hands down. It’s not even close by anyone else.
I think the worst is HUGO. And yesterday I understood - it’s not the cart that’s the issue - it’s actually probably a non issue. It’s the payload and big arm. The areas of movement are way too big.

“But that gives stability” - I’m going to burst that bubble in a minute. Because the carts of HUGO are big and solid and do not move. Mass and stability - 100% brilliant. Instrument shake and “wobble” - a very minor issue for HUGO - that has nothing to do with the arm stability in my opinion. (Let me come to that later.)
So what does this mean. Because this is the crux of the issue with HUGO in my opinion. But issues that absolutely can be overcome. All of that hardware up above the patient can become a nightmare for clash - reach issues - beside assists. Because if you set that up wrong the issues will be amplified by the arm design. But. And this is what I want you to take away…. BUT if you set it up right - and I saw yesterday - it becomes an absolute non issue. Yep you read that right. Set up right and the issue with all that mass and size above the table goes away.
With Prof Rottoli understanding the physics and “air space” of the arms - in a very complex multi docking procedure - there was not even close to a single clash. Not One !
There was never a single moment where instruments clashed inside. Not one moment where the scope couldn’t reach. Not one instance of instruments not being able to reach. Not one. And that is where the lightbulb went on.

And I can assure you 100% it is all down to a fundamental understanding of the issues of the arm - and then being intelligent in setting up port positions (fairly laparoscopic) and then setting arm heights - joint angles and most important “ARM ROTATIONS” to allow full range of motion without interference.
(This is just my opinion) I cannot stress enough to everyone - if you try in any way to set this up like any other robot. You will fail. If you put ports like a da Vinci - you will fail. If you neglect to set each arm to a particular range of free movement - you will fail.
This masterclass by Prof Rottoli and his team (including the Medtronic clinical team - which I’ll talk in details about later) was a demonstration that I feel all Medtronic users should be exposed to. (Maybe they are? But feedback would say they are maybe not.)
Surgical companies can all too easily think about what’s happening “inside” the patient during set up and use. Focusing on testing reach and movement inside. Because that has been the focus for 30 years in lap. You don’t need to even think about the arms of a surgeon moving outside - it just happens. With HUGO - just because of the design - for me it is all about the outside airspace set up. This is counter intuitive for most companies.
The downside of HUGO are the massive arms - but that can actually be turned into a strength if you are smart. And you are patient enough to understand the arm geometry.
Why? Because you have so much flexibility - reach and movements - that you can be very flexible in arm set up. And just forgetting everything you have ever learned about da Vinci is critical to get HUGO to sing. (My very humble opinion.)
But it would explain to me the surgical feedback I’ve had over the last few years. Especially from urologists who say “it doesn’t work.” They need to say “It doesn’t work if you try to use it like a da Vinci.” And they’d most likely be right.
I can already imagine that in renal cases - if you think like da Vinci and get fixated on one dock only arm position - you will be frustrated as you move from north to south poles of the kidney. I have no evidence - but seeing this yesterday I could visualise a 3 arm renal case and think of a da Vinci style set up; and a user being pissed off at arm movement and clash. I think it will be obvious.
So. Get a masterclass in set up - it’s fast - easy - and once it is set right - you will have no issues with clash or instrument reach. But… (and this is a very big but...)
Don’t be scared to re-dock
One of the downsides of doing Z-rail to port docking is that you automatically think da Vinci. And too many people think - “Docking more than once is a failure often requiring more ports and losing time.” We all have to get out of this one dock mindset for modular arms.
Modular robots offer something boom robots do not in docking and set up. The ability to move the fundamental starting point of the arm - the base cart - joint Zero. And unlike a da Vinci you can move all 4 independent of each other. If you do not use this phenomenal feature (of all modular robots) you are missing the main point of modular.

You can use the same ports (as I saw yesterday) but re-dock with different arm set up and get way more comfortable and clash free reach. Stop being scared to dock and re-dock.
No human bedside assistant stands in one spot and never changes arm angles - and tries to do the whole case from an over reaching position. Think of modular carts as one arm assistants - and let them move if they have to - to be more comfortable. MOVE!!!!!
I imagine that if you are doing the angle by angle - degree by degree - set up as per the HUGO manual in your case number two or three - and it is taking time to dock. You will be terrified of undocking and then going through all that pain again . It’s unthinkable. Especially for da Vinci users that have mastered a single dock. The user will resist with every fibre in their body to undock and re-dock. And that is where problems will occur.
This is all about docking education. The team must get fluid and fast and not be scared to re-dock. In my view this is the way you get clash free procedures - maximal internal reach and instrument clash avoidance. Think laparoscopic! Not robotic with HUGO was my big takeaway.
To that end - if anyone from Medtronic is reading. Here’s my thoughts. Please for now - don’t focus on da Vinci urologists. Doff your cap - but trying to win them (I think) will be your undoing. This ain’t a da Vinci - and they are not you heartland customers.
You have to be able to do urology - it MUST be cleared and able to do prostates - but NOT focus on it. Again just my very humble thoughts.
Tower and set up screens.
My first time looking at all that info - and setup buttons and all kinds of graphics etc etc; It felt a bit bewildering. I can imagine some OR teams may struggle at first with all that engineering stuff. But I could be wrong here - just my initial feedback was “This was designed by engineers not people that live in the OR.”

But hey. Just trying to give my full view. Because the whole user experience is just - to me - industrial. It is so unnatural to hear these sort of machine shop clunks and bangs as arm mechanisms seem to engage and disengage. Felt like it was the loader from Aliens the movie. Dunk - move Clunk - move.
So many buttons and interfaces on the arm. Engineers wet dream and nursing team’s nightmare.
Such an odd design philosophy.
Hey I’m an iPhone guy….
That design philosophy also seems to overflow to the massively oversized lap tower. It feels - well old and out of place. Like a big computer rack with space to fit other people’s stuff on it. And fit it badly. Not nicely fitting Storz equipment - but empty shelf space. Again - must be for upgrades later - but it just feels bigger and bulkier than it needs to be and sort of “an add on.” If you compare to a DV5 tower - it’ not even close. Again just feedback - didn’t impact the case - but just not something I’d rave about. Great solid connects - cables - buttons - well built but poorly designed would be my summary. Engineering choices?
The HUGO RAS console
Now this is where I just wonder if an entirely different company built the console. It’s simply gorgeous and incredibly functional.
Let’s start with the Eizo screen - it’s big - it’s bright - it’s HD - it has great 3D. The size just feels perfect where you can see enough but it doesn’t create peripheral vision issues. And what I do like about the screen is the GUI. I noted there was virtually no graphics interfering with the surgical view. That in great part is because they had the sense to have a very very nice “wing mirror” display. Where a lot of control and functions are right at the user’s fingertips.
There were only two mini alerts / alarms in the day. One was a bipolar issue that got alerted as a user “watch out”. The other was the bedside team had leaned on an orange “anti finger trap” bar safety button. And that set of an alarm for the user.
Prof was very quickly able to touch the wing mirror and silence the alarms - and continue. That interface is very very nice. The wing mirror is smart.
The design cues of the console are just so removed from the arms. It’s elegant - slim - spacious and really well thought out. The arm carts (bases) are closer to console design cues - but then they have that industrial era factory arm bolted to it.
On the console, the bottom mounted haptic arms are amazingly slim and elegant. No big bulky motor drives or complex cabling. They are super sleek and functional. They terminate in the hand controllers - which are small pistol grips with a lot of functionality. I dare to say - the best handgrips in the business. Especially if you are a lap surgeon - this will feel like home.
Now we can discuss hand orientation vs instrument line up later.
But this combination of elegant haptics and handgrips, I think, is the industry best to date. A lot of thought has gone into them. They are conformable, and I could see the slim design looks way more ergonomic than any other controllers - and I think hand pain will be low risk with this set up.

The haptics are super fluid and silent - and what I noticed (in part because of a skilled user) was that they got the scaling right. The hand movements are very controlled, to translate to excellent instrument movements. The amount of movement, the degree of rotation - the articulation just worked so well in combination. Lag was very low. And the movement volume was well… just spot on. No need for wild hand movements at all. Great relational mapping to the instruments.
I was so enthused by the console experience. (And that is where you will win the heart of the surgeons as that is what they really interact with.) It all had the right combination of hand vs foot controls. The pedal deck is again probably the nicest and best looking pedal deck in the business. Well laid out - nicely fluid - camera and clutch control excellent.
Plus it has the instrument controls for electrosurgery etc - Well laid out and design wise gorgeous. Great coloured halos and sizing seemed spot on. It is clear that the human factors team on the console really understood what they were doing. There is one small snag - one annoying thing. You have two big foot pedals for Ligasure cut and seal - that are just begging to be activated. Where the hell are the instruments???? There are two giant illuminated signs screaming at the user.

When you put this entire console experience together - and how they have fine tuned it. I’d say that the console experience maybe the best I’ve dealt with so far in our industry. I’ll apologise now to Medtronic for all my other rude stuff - as the console is excellent.
Vision and accessories for HUGO RAS
If you are going to roll out two parts of your hardware arsenal that are just going to be great - no doubts, Slap on a STORZ vision system and a Valleylab generator. You cannot really go wrong.

HUGO has a Storz HD 3D system - (I hope they get Rubina soon for ICG) - and a EIZO HD 3D screen. The combination is lush. Prof demonstrated panoramic views to super close in with zero focus needs. The German’s just firkin know how to do this well. Colour rendition is great - illumination is good. Resolution (even with 3D glasses and 3D screen is great.)
But what laparoscopists should love is their retained, standard field of view. This is a STORZ laparoscopic imaging system, so based off their hand held optics. That means what you get in lap you get in HUGO.
I’m not going to do this justice here so apologies up front. Any robot that maintains standard laparoscopic fields of view - I think - will always feel more familiar to laparoscopists coming into the fray. It feels like home. If they have to switch to a new angle or field of view that is not what they’ve been watching for the last 20 years - it’s more learning curve.
As a side note: Same for the port positions. If your angle of approach is changed to be more parallel than you’re used to - it takes adaptation. If (like most modular robots) you can stick your ports in a familiar place. Then you know when an instrument comes from that same angle, from that port site (because you’ve done it of 20 years) it helps the learning curve. Trust me I’ve seen it first hand.
So Medtronic having this Storz system felt like home to someone like me that loves laparoscopic vision systems..
Energy: Now- advanced energy is a major major topic. And why there is not at least a straight Ligasure hanging from a HUGO (clinically) is just baffling to me. (Okay it’s priorities - regulatory etc etc I get it.)
So if my armament is diminished, I need to have bullet proof bipolar and monopolar.
In steps - arguably the best electrosurgery generator in service today - Valleylab FT10.

The electrosurgery delivery and coagulation functionality throughout the whole procedure was impeccable. They have done a great job of marrying up instrument electrosurgery performance with generator delivery - and GUI cockpit feedback. The switching between monopolar and bipolar was fluid. Power setting perfect. This is where you get massive integration benefits when a single company owns the whole chain - generator - software - robot - instruments.
In fact in the hands of Prof Rottoli yesterday you might ask “Do we even need an advanced energy?”
Outcomes wise no. But speed wise it would be a very nice tool. But in its absence I could not find a single fault with their ability to deliver highly controlled energy.
The combined Airseal made smoke no issue and the view was crystal clear at all times. (Medtronic - get your own insufflator.)
I’ve got to give HUGO 100% on electrosurgery deliver via their instruments.
Stapling: Now during the case we did use a stapler. It was not a robotic stapler - and a very very capable bedside surgeon (Giacomo Calini) was able to fire the Medtronic hand held; and it was quick and easy. Access was a little bit harder for the bedside due to the real estate above the bed - but could it be done. Yes.
A robotic stapler in this case would have also worked a treat - and would have eliminated the need for the “Left a bit - no pull back” dialogue between the console surgeon and the bedside. I think the robotic surgeon control of the stapler brings another dimension. Especially if you don’t have such a talented bedside surgeon. Can it be done manually - yes. If there was a robotic option available on HUGO at the same cost - would Prof have fired it himself? I’ll let him comment.
Access: Trocars were the usual bullet proof construct of Medtronic. If with the heritage of USSC they can’t make trocars then we are all doomed. But. One of the oddest things I saw was a lack of a 12mm robotic port. They had 8mm for the instruments and an 11mm for the scope. But for the stapler? Or the 12mm clip appliers? Maybe it was just me, but it seemed an odd oversight.
I quite liked their round docking clips to the port. Firstly you can dock in to the port from any angle. Next you can swivel the ports the get the luer gas connectors out of the way. Being picky...I would like to see some ports with no stopcocks - to stop accidentally getting in the way or digging into the patient. Just a minor gripe - but it's the small things that make the difference in robotics.
HUGO RAS Instruments
For me - one off the single most important parts of any robotic system are the good ole knife and fork - the instruments.
This has been the bane of every (including Intuitive) surgical robot when they start. No one has been immune. Be it performance - availability - breakage - costs - cleaning - you name it.
Because wristed instruments are bloody hard.

So my beady eye was looking very hard at the instrument performance of HUGO during a fairly tough case. I was looking for build quality - tip apposition - cable fray - energy delivery - accuracy - sharpness - grip strength and a whole host of attributes that are important to the user - and have been reported as issues in the past.
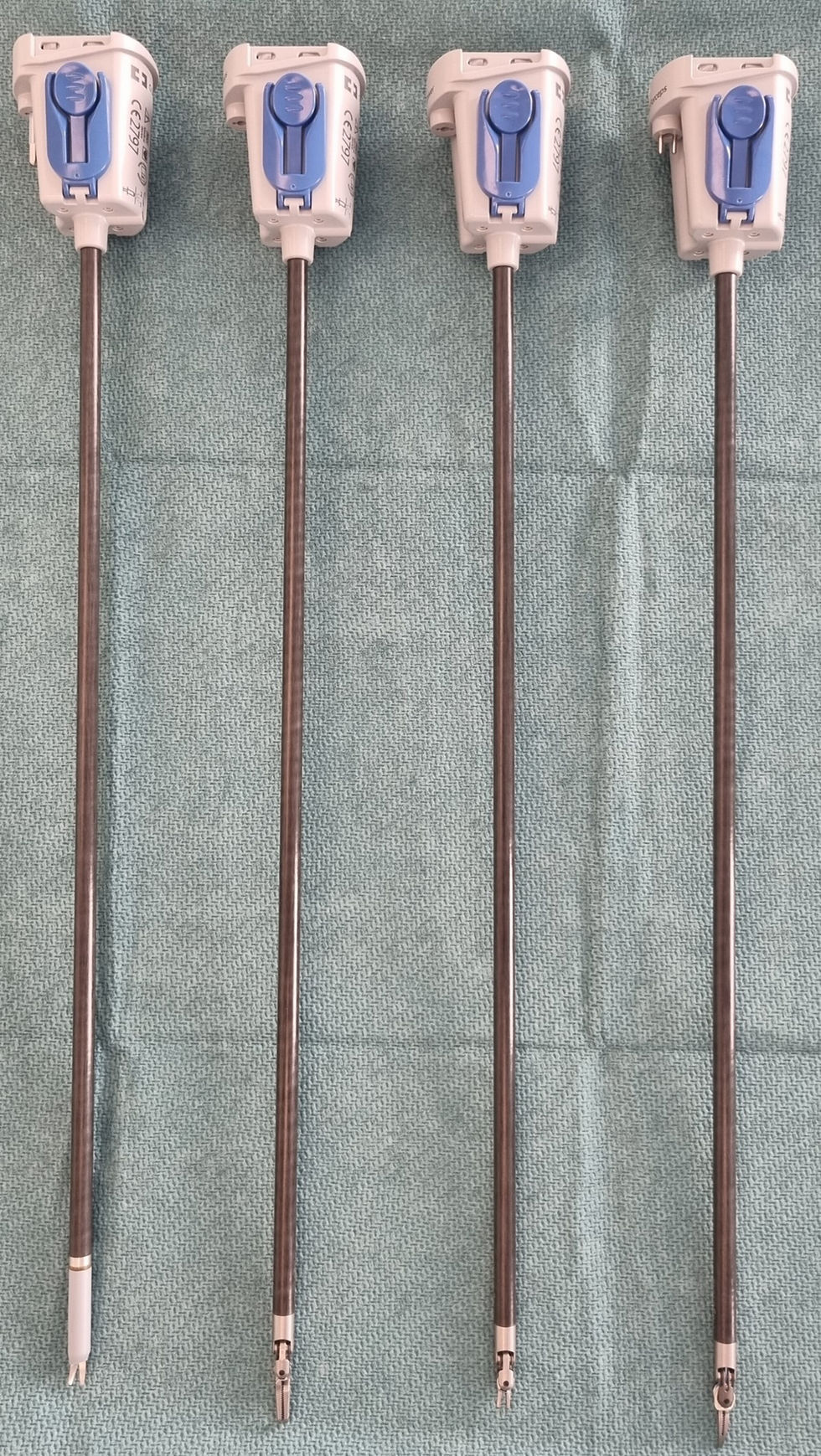
Let’s start with the grasper (Cadiere) - I can only say - Brilliant. Super strong grip force, phenomenal fine tip grasping and (as expected from such big strong arms) lifting power was everything it needed to be.
Articulation was spot on - and at no point did I witness any struggle in any aspect. Looked pretty bullet proof to me.
Bipolar graspers. Great build - very robust. Great tip grasping (important) - near perfect jaw alignment - ample strength. And most importantly - super super good bipolar delivery with little to no tissue eschar. Valleylab knowledge shining though there. Really spot on.
But.. what about scissors - the weak point of any instrument line up. Well.. the sheath fitted brilliantly - and was flexible with only some slight folding. Instrument scissor tip was long enough and passed the protective cover adequately. Jaw opening was good - and cutting to the the tip was hyper precise. Application of monopolar was again excellent for both cut and coag (and super easy to flick between both for the surgeon.)
The lower time of use duration per case is the only niggle I’d have - but in a cost per case model - that’s Medtronic’s issue not the customer or surgeon.
Performance wise, a really really precise and good scissor. Not one bad thing to say about its performance.
Have I been lucky? Am I just seeing the latest variants? Maybe. But as an impartial report - the instruments performed as well as da Vinci (from what I see) but maybe even better on electrosurgery. It just felt “lower energy” and higher control for the electrosurgery. What I expect from Valleylab know how.
Okay - you’re all sick of me being so positive - so let’s talk for one moment about instrument judder. As with quite a few of the newer systems - when the surgeon engages and makes the initial move - or stops a movement - there is sometimes a little bit of instrument wobble.
On HUGO it’s there. It’s a launch and stop issue. During the movement it looks super smooth - and during usage it looks super accurate and smooth. But it has that slight shake when it sets off or stops.
The uninitiated may say - “Ah well that is because the carts are single arm carts and not heavy and stable enough. It’s a problem of arms.”
No. Not from where I was sitting. I watched very very closely. Those arms are very big - very heavy and very stable. I would offer up that this is a software control problem. It’s tiny, but it’s in the software as far as I can tell. Some kind of feedback issue - or hysteresis of the trocar valves on the instrument shafts. It’s minimal - but it is there. I think it can be fixed through software. But it didn’t affect the accuracy of the instruments in use. However it makes a system feel less solid and accurate compared to a daVinci. DV5 has none of this. It’s buttery.
HUGO absolutely misses an electrosurgery hook for sure. And I didn’t get a chance to see suturing so next time I’d love to see needle holders and how well they work. Especially the mapping during suturing manoeuvres.
But from what I saw - good solid quality instruments - nice simple side loading - great articulation - good precision. Great reach and solid strength. Full marks. No much for me to moan about.
Instrument control on HUGO RAS
I sort of mentioned this earlier that the haptics and hand controllers are great. But I think I saw something that I think might frustrate some da Vinci users that use the finger pinch controller paradigm. I noticed that often the alignment of the operator hands and axis of the controllers was often not aligned to the instrument tips. They were sometimes up to 90’ off axis.
It was super clear to me that Prof Rottoli had already compensated for this in his mind through so much use and cases. But he is not a former da Vinci user - and I’ve seen this myself - that when a “no robotic user” gets on a system as a virgin - and adapts to the controller mapping - they learn faster that control paradigm and have less issues. But often a da Vinci user will struggle if the hand controllers are different. They will complain. They are used to the axis of the hands lining to the axis of the instruments.
All other aspects of instrument control and lag - and precision were great. It was just an observation I made. And I'll repeat - they nailed scaling. At no point were hand movements excessive to get the required instrument movement.
Now, how was I able to see the screen - and the robot arms and the hands of the surgeon??? Well open console my friends. That is one of the massive advantages - teaching and observation. Just saying. Just saying.
Medtronic OR Support team
Surgical robotics is not just about the surgical robot. It’s way way way deeper than that. And one of the most critical parts of a successful robotics program is the in OR support of the company's clinical specialist. I had the pleasure to meet the team from Medtronic at Sain’Orsola that supported cases there.
They were incredibly professional - knowledgeable - courteous and an integral part of the smooth flowing of that program. What is clear to me is that they were experts in HUGO and were able to assist without being in the way... and just make the whole case more fluid. And that’s a testament. That is why you need them.
What was important is that at this stage of the learning curve - that Medtronic team is not needed there all day every day - which is critical if you want to scale programs. It was obvious that Medtronic had trained that Sant'Orsola OR team well - but it was more obvious that OR team were the people “teaching” Medtronic in many respects. I’ve been in enough cases where I know the dynamics, and it is very clear that Prof and his team have worked the dance out for the system and have fed that back to Medtronic. Which - by the way - is the right way. Two way communication and learning and then dissemination of those learnings.
I would like to say thank you to the Medtronic team there for tolerating my presence, being super polite, and answering my non confidential questions. They were a credit to Medtronic and our industry as a whole.
But what it highlights is how critical that investment into that team is. And getting the right skilled people to do that case support. It’s a big expensive investment that all companies are going to work out sooner or later. And not only that - there are not that many of those people just “hanging around” the best are all being scooped up by the companies. Whoever comes late to this dance is not going to find these essential clinical specialists. The people that make the difference in those cases like yesterday.
All robot companies - prepare to invest BIG TIME in these OR support teams.
Why I think many surgeons will struggle with HUGO
This is all wild speculation from observation so take it as it is:
I want to drop out of observation now and more into philosophy. Prior to seeing this case I had wondered “Why do so many struggle? So many reportedly send systems back? Have issues? Yet others are having glowing reviews?”
This was a fundamental question that has bugged me about HUGO. Medtronic are not a start up - so it is not related to that. Yes there will always be a few quality issues at the start… normal. But this to me has been something else. If everyone getting on HUGO was able to run it like Prof Rottoli - then there should (by now) be hundreds and hundreds of happy and active systems and programs out there. And as far as I can see… there are not. Why?
For me it has become entirely obvious in this one critical experience.
It’s the airspace management above the patient at docking that is the key for me. And that requires a very very specific training - patience and type of user. I’ll repeat. And this is just my observation. If a da Vinci user tries to replicate a da Vinci use. It’s doomed.
If a lap user wants to put in the trocars and just connect the arms and go. It’s doomed.
This initial dance - where the ports are placed and then each arm tailored to the port in relation to the other arms - for motion - clash and reach - is a step that da Vinci users don’t need to do (They can almost just follow the diagram) and many lap users will not have the patience to do all that set up. And it is NOT about the instruments inside… it’s outside.
The hardware is so big above the patient - and the margin for error so small - that the “pre dance” is critical.
And then... If you hope for a single dock - in many cases it’s doomed. Maybe single pelvic case or a simple inguinal hernia - and upper GI Nissen. The single arm geometry set may work. But multi quadrant - I think a dual or even triple dock will be needed (not new trocar places necessarily) but totally new arm poses. If OR teams don’t have the patience to do both of these things, then I think HUGO will be working sub optimal. Leading to problems.
Watching arm speeds and momentum - I would not want to see two drive units smash into each other. If that happens it could be an alarm - a damaged arm and a reboot. And if (sorry I don’t know) there is no hot swapping, then that is a set up recycle and that can be 20 minutes plus. That will infurriate any team going through a learning curve. Prolonged anaesthesia time is tolerated to a certain degree.
Arm setup issues will result in Instruments not feeling like they are working well. Small issue upon issue piles up - it's "a small stack that gets heavy." All derived from that limit of airspace and lack of set up curation. It’s weird I know - but this is how perception builds and frustrations mount.
Knowing how kinematics also work - I just have a tiny suspicion that if you start to get the carts too far from the table - that will compound the issues above the table. I’d have to play with set ups to be sure - but something tells me the further away… the more joint movements you might need so more clash? What I saw was that yesterday the close in compact set up compressed joints and seemed to tame the need for excessive movement. Perception?? Maybe.
If surgeons do not spend 90% of their time training on the “outside above the patient” my gut tells me they will struggle with HUGO. I know surgeons want to get in and get cutting. But something deep inside me tells me - with HUGO it’s all about the outside. And I'm not talking about the floor space - it’s the volume above the patient. It’s knowing about twisting arms though 90’ and making joints work horizontal not vertical. It’s about thinking in 3D and getting height clearance between arms not just X&Y. It's about making sure arms miss each other.
And through my own experience - a lot of surgeons are not going to put that learning effort in. They are not going to heed the “Please don’t do a da Vinci trocar placement and arm set up.”
In my humble opinion, this is not plug n play for a current robotics user. And if they want to jump into 4 arm procedures (3 instruments and 1 scope) - with these long Z rails - that is a world of hurt waiting to happen.
And unfortunately hospital management will be saying “you can only use it for the most complex cases” compounding the whole issue. It would be way better for 3 arm simple procedures and a gradual understanding of the kinematics of the arms and airspace management.
I would love to look at the user experience and telemetric data of prior DV users vs non DV users on HUGO. Also those that work out the arm set ups tailored by case - and those that follow basic instructions. I think it would be fascinating.
One warning I will give is for the USA. I fear that the patience and time set up for US hospitals - and US users that are all deep DV surgeons are going to compound this issue. This could be difficult. I’m putting my US hat on - and imagining the first 10 cases with a few people I know…. Yikes.
I would be paying super close attention to have all my early users to come and see Prof Rottoli and get that airspace explained. What he showed me yesterday - in my simple mind - is a critical success factor with HUGO and its current design. Pay the air tickets…. :)
Design updates to HUGO RAS needed?
I’ve been around robots for a few decades now. I’ve seen hundreds of labs and hundreds of cases. I’ve sat and driven most systems. I think (because I’m stupid and arrogant) that I know what a good robot needs to do. Depending on its architecture type.
For me - from what I saw - HUGO actually has a lot of merit. (Shock gasp I hear!) But like everything in life, it comes with a ton of caveats.
I think they’ve nailed the console - Instruments are great - Energy - world class. Carts - are not as big an issue as I would have said 48 hours ago. You can live with them... if you’re smart.
But it’s the arms and the drive packs. I think Gen 2 needs to make these compact - lighter - and easier to use (cobotic) in setup. It also needs to be more forgiving in set up. Get the engineers out of the room for a while and get better usability clinicians (nurses) in.
In general, a simplification is needed. There should be no need to know angles and gauges and buttons and complex set ups. A high focus on the user experience of the arm - to match the user experience of the console would be ideal.
In the interim I’d be highly focused on air space training, picking the right lap surgeons, avoiding urologists, getting 3 arm procedures going first as a learning curve and being strongly open that “You cannot use this like a da VInci." Well that would be my plan.
I am positive Medtronic already know this and they are probably way ahead of me. But just giving my thoughts.
Summary of my day with HUGO RAS
Being honest - on the train heading from Rome to Bologna - I was confused as to why Prof Rottoli was doing so well - and so many others were belly aching. I wasn’t that enthused to go and see a lumbering robot set off some alarms - have instrument issues and software bugs.
But coming back on the train I was suitably impressed with what I’d seen. Hugo (when used this way) didn’t feel so big. Yes the air space was and is still a weak point - but I’d seen how when it’s managed the right way - it can become a relative non issue. I think this was both the surprise that delighted me - but the insight I needed to rationalise this polarity of experiences out there. Maybe I’m wrong - but in my head I now “get it.”
Lots of strong points for them to build off - console - electrosurgery - imaging… and I have to say - pretty decent instrument performance.
When I’m tough - it’s really not because I’m being an ass. I’ll say it until I’m blue in the face. Medtronic and JNJ cannot fail in surgical robotics. And today I came away a little more hopeful that Medtronic has a decent base to work from. No doubt in my mind they have a ton of work to do. They need to redesign that arm. They need to focus outside not inside until they redesign. They need to pick their surgeons very well.
I love to be proven wrong - today I admit I'm partly wrong.
Also - my sincere thanks to Prof Matteo Rottoli for letting me into his OR to see HUGO. It is always a privilege to see a very skilled and talented surgeon operate. And Medtronic should be super proud to have him as a user of HUGO.
These comments are the author’s own and independent opinions and this piece was not in anyway organised or paid for by Medtronic. This was an independent visit to Bologna to the department of surgery under the invite of Prof Rottoli. These views are for educational purposes only and do not reflect the views of Prof Rottoli, the Sant’Orsola or Medtronic.